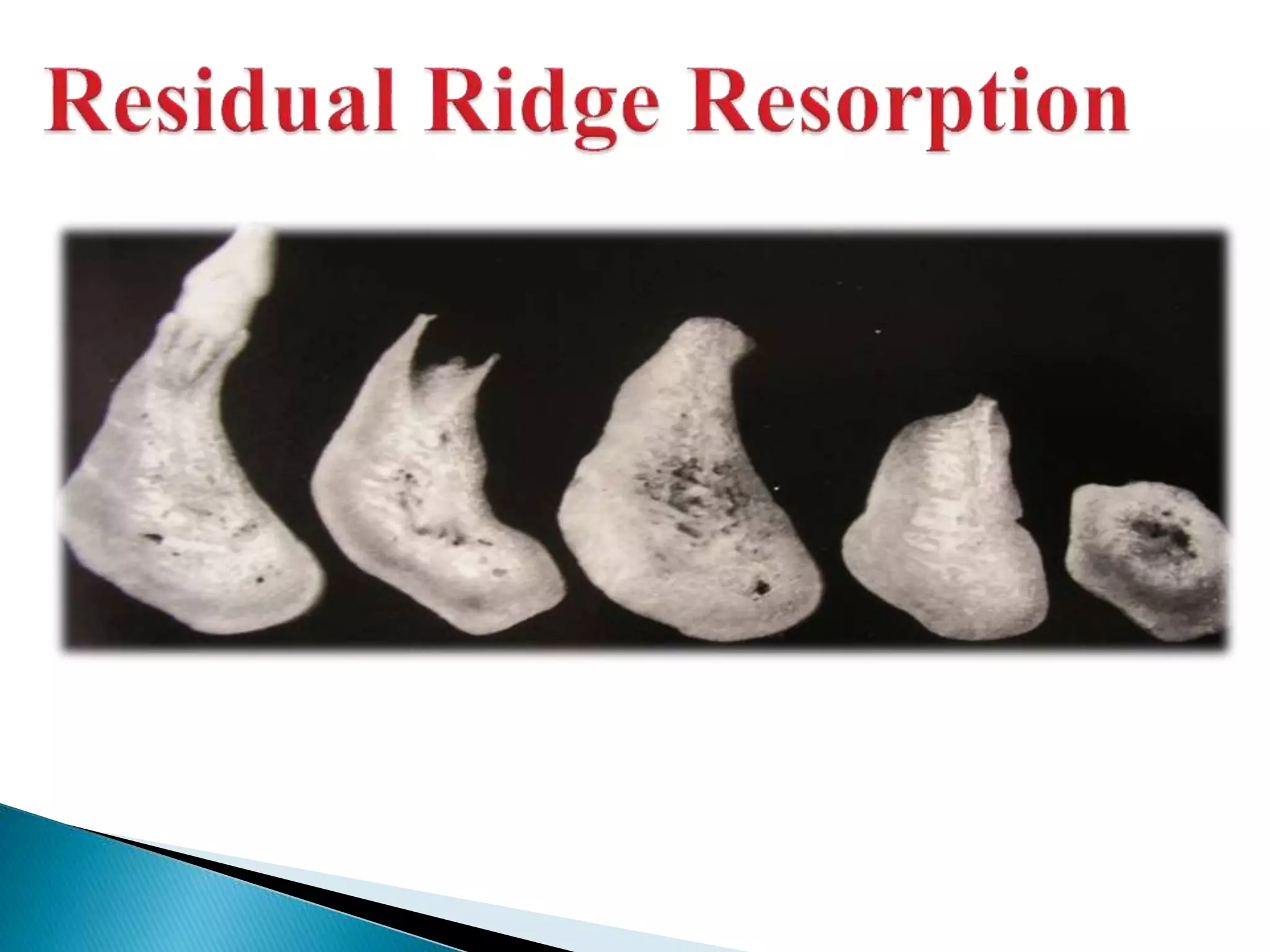
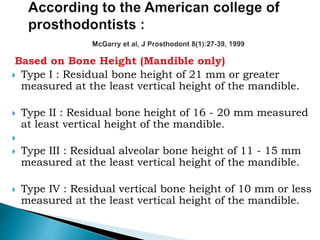
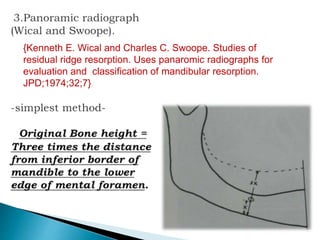
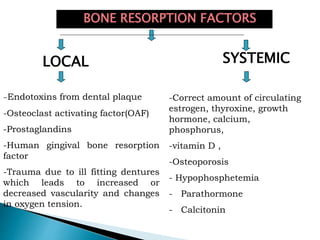
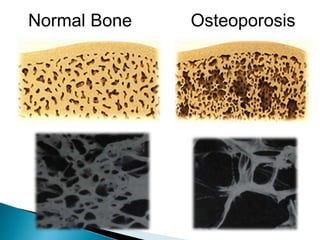
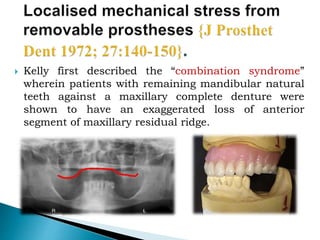
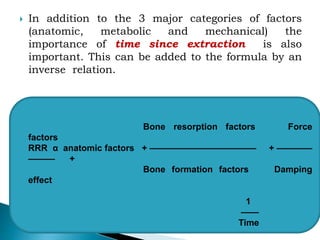
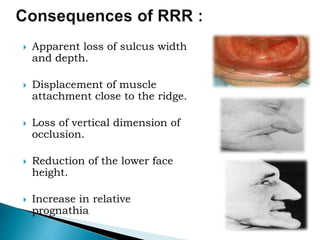
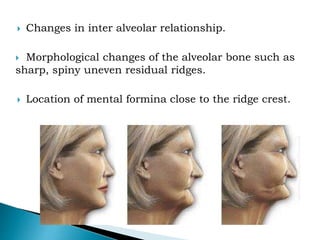
The document discusses residual ridge resorption (RRR), which is the progressive loss of jaw bone after tooth extraction. It defines RRR and provides classifications. RRR is considered a pathological process due to its variability between individuals. The document covers the epidemiology, etiology, and risk factors of RRR, including anatomical, mechanical, metabolic and prosthetic factors. Treatment aims to prevent or reduce RRR through denture design and patient education.


![DEFINITIONS :
“Bone - a highly vascularised, living, constantly
changing, mineralized connective tissue”. [Gray’s
Anatomy-40th edition]
“Alveolar process -- that part of the maxilla and
mandible that forms and supports the sockets of the
teeth”. [Orban’s]](https://image.slidesharecdn.com/residualridgeresorption-150906071207-lva1-app6892/85/Residual-ridge-resorption-3-320.jpg)
![ “Alveolar bone is the bony portion of the maxilla and
the mandible in which roots of the teeth are held by
fibers of periodontal ligament”. [GPT-8]](https://image.slidesharecdn.com/residualridgeresorption-150906071207-lva1-app6892/85/Residual-ridge-resorption-4-320.jpg)
![ “Residual alveolar ridge is the portion of the
alveolar ridge and its soft tissue covering
which remains following the removal of or loss
of teeth.
[GPT-8]](https://image.slidesharecdn.com/residualridgeresorption-150906071207-lva1-app6892/85/Residual-ridge-resorption-5-320.jpg)



























































![residual ridge resorption seminar final [Autosaved] latest.ppt](https://cdn.slidesharecdn.com/ss_thumbnails/residualridgeresorptionseminarfinalautosavedlatest-250220070708-69d45f3c-thumbnail.jpg?width=640&height=640&fit=bounds)















![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









