Case presentation -group-14--20160520
•Download as PPTX, PDF•
2 likes•861 views

This 71-year-old man presented with gross hematuria and a bladder mass. He had a history of asbestos exposure and other medical issues. Evaluation revealed a large fungating bladder lesion, and biopsies confirmed adenocarcinoma. Further testing found prostate cancer involving 30% of tissue with a Gleason score of 7. The tentative diagnosis was urothelial carcinoma of the bladder neck, prostate urethra, or both, but immunohistochemical staining was positive for PSA, suggesting the final diagnosis was prostate adenocarcinoma with invasion into the bladder.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Case presentation -group-14--20160520
Similar to Case presentation -group-14--20160520 (20)
More from PoKai Chan
Recently uploaded
Recently uploaded (20)
Case presentation -group-14--20160520
- 2. Chief problem History Personal, Past, & Family Present illness Physical examination Review of Systems Lab data Tentative diagnosis
- 3. Chief problem A 71-year-old man had gross hematuria and a mass in the bladder
- 4. Chief problem History Personal, Past & Family Present illness Physical examination Review of Systems Lab data Tentative diagnosis
- 5. Personal history • He was married, had adult children, • retired from the shipping industry, • where he had been exposed to asbestos. • He was physically active in outdoor activities.
- 6. Past history Erectile dysfunction Hypertrophic cardiomyopathy Diverticulosis Obstructive sleep apnea Nephrolithiasis (had treated) Hypertension Hyperlipidemia
- 7. Past history • Results of a colonoscopy performed 1 year earlier were normal. • Medications included atorvastatin and verapamil ; other medications had recently been stopped. • other medications : doxazosin, amlodipine, valsartan, telmisartan, hydrochlorothiazide, potassium aminobenzoic acid, oxybutynin chloride, and potassium chloride supplement • NO smoke & NO alcohol
- 8. Family history There was no family history of urologic cancers.
- 9. Chief problem History Personal, Past, & Family Present illness Physical examination Review of Systems Lab data Tentative diagnosis
- 10. Transurethral resection of the prostate :because of lowerurinary tract symptoms and urinary retention. Pathological examination of the tissue reportedly had shown an area of focal high-grade prostate intraepithelial neoplasia. prostatic biopsies : negative .Four subsequent prostatic biopsies, the most recent performed 4 years before Results of a colonoscopy were normal 12 years ago 4 years ago Present illness 1 year ago
- 11. gross hematuria(血尿) and a mass in the bladder for 6 weeks painless hematuria had developed, with passage of clots prostate-specific antigen (PSA):13.0 ng per millilite CT :After 2 days,computed tomography (CT) reportedly revealed a multilobulated(多房性) mass (isodense to hyperdense and measuring 8 cm by 7.5 cm by 6.5 cm) in the urinary bladder, diffuse fat stranding in the perivesical and left periurethral regions, and bilateral intrarenal calculi(結石) and cysts cystoscopic examination:The next day, cystoscopic examination revealed an open prostatic urethra and brisk(輕 微) bleeding. A fungating lesion at the anterior bladder neck at the 12 o’clock position, with an adherent clot, was partially excised. Pathological examination of the tissue reportedly showed focal adenocarcinoma in situ Two mons ago 3weeks ago Present illness 1 mon ago
- 12. Ultrasonography of the abdomen and pelvis revealed bilateral renal cysts and bilateral nonobstructing nephrolithiasis The next day, repeat cystoscopy reportedly revealed a large fungating lesion and clot at the anterior bladder neck at the 12 o’clock position. Flushing of the bladder and biopsies were performed. Pathological examination of the biopsy specimens reportedly showed adenocarcinoma; consultation with outside experts was pending. CT of the abdomen, performed the next day, reportedly revealed no evidence of metastatic disease. After decompression of the bladder with a catheter(導管), irregular thickening of the bladder wall was seen, with an irregular, multiloculated gas collection, 2.5 cm by 3.5 cm, in the suprapubic(恥骨) region. 2 weeks ago Present illness
- 13. Transrectal biopsies of the prostate with ultrasonographic guidance: adenocarcinoma in one of two cores from the right base, with a Gleason score of 7 (grade 3 plus grade 4) on a scale of 1 to 10 (with higher scores indicating a worse prognosis), involving 30% of the tissue, and adenocarcinoma in a core from the left lateral midportion, with a Gleason score of 6 (3+3), involving 10% of the tissue. Present illness 5 days after 2nd cystoscopy
- 14. the pulse was 50 beats/min and the blood pressure, temperature, respiratory rate, and oxygen saturation were normal. Rectal examination was not performed, and the remainder of the examination was normal. Blood examination K+ 3.3mmol/L(3.3-4.8) creationine 1.3mg/dL(0.6-1.5) Urea nitrogen 15mg/dL(8-25) eGFR 59 ml/min/1.74m2 (>=60) The complete blood count and levels of other electrolytes, calcium, and glucose were normal. Present illness This evaluation
- 15. Chief problem History Personal, Past, & Family Present illness Physical examination Review of Systems Lab data Tentative diagnosis
- 17. Review of system CONSTITUTIONAL HEENT RESPIRATORY BREASTS CARDIOVASCULAR GASTROINTESTINAL GENITOURINARY MUSCULOSKELETAL NEUROLOGICAL PSYCHIATRIC SKIN ENDOCRINE/ METABOLISM HEMATOLOGIC ALLERGIC AND IMMUNOLOGIC ● No night sweats. No fatigue, malaise, lethargy. No fever or chills. ● Eyes: No visual changes. No eye pain. No eye discharge. ENT: No runny nose. No epistaxis. No sinus pain. No sore throat. No odynophagia. No ear pain. No congestion. ● No breast pain, soreness, lumps, or discharge. ● Mild obstructive sleep apnea No cough. No wheeze. No hemoptysis. No shortness of breath. ● Hypertrophic cardiomyopathy, hypertension ● Diverticulosis No abdominal pain. No nausea or vomiting. No diarrhea or constipation. No hematemesis. No
- 18. Review of system CONSTITUTIONAL HEENT RESPIRATORY BREASTS CARDIOVASCULAR GASTROINTESTINAL GENITOURINARY MUSCULOSKELETAL NEUROLOGICAL PSYCHIATRIC SKIN ENDOCRINE/ METABOLISM HEMATOLOGIC ALLERGIC AND IMMUNOLOGIC ● No musculoskeletal pain. No joint swelling. No arthritis. ● He had an episode of mild confusion. He has chronic right hemiplegia. No headache or neck pain. No syncope or seizure. ● He gets occasionally confused. ● No rashes. No lesions. No wounds. ● No urgency. No frequency. No dysuria. hematuria. Lower urinary tract symptoms, urinary retention. Erectile dysfunction, nephrolithiasis No discharge. No pain. No significant abnormal bleeding ● No anemia. No purpura. No petechiae. No prolonged or excessive bleeding ● No pruritus. No swelling.
- 19. Physical examination • PE by Dr. Donald S. Kaufman – HR: 50/min, blood pressure, temperature, respiratory rate, and oxygen saturation were normal. BMI: 30 – Rectal examination was not performed • PE by Dr. Olumi – Digital rectal examination: the rectal tone was intact, the pelvic organs were mobile, the prostate weight was estimated to be 40 to 50 g, and there was no palpable prostate nodule or rectal mass. admissio n
- 20. Chief problem History Personal, Past, & Family Present illness Physical examination Review of Systems Lab data Tentative diagnosis
- 21. Laboratory data • CBC and other electrolytes, calcium, and glucose;Cr、urea nitrogen were normal Abnormal blood potassium 3.3 mmol (3.4-4.8) eGFR 59 ( ≧60)
- 22. Laboratory data
- 23. Laboratory data
- 24. Chief problem History Personal, Past, & Family Present illness Physical examination Review of Systems Lab data Tentative diagnosis
- 25. Tentative diagnosis Urothelial carcinoma of the bladder neck, the prostatic urethra, or both. But after Immunohistochemical staining P63 - PSA +
- 26. Division of work Yao Chung-hsia Yu Hung-Chun, Li jia-xuan, Li ho Lee Yi-zhang Wu Zon-han Chan Po-Kai
- 27. Thank you for your attention
Editor's Notes
- Asbestos 石綿
- 為什麼做bone marrow biopsy? Finding的涵意是?
- 為什麼做bone marrow biopsy? Finding的涵意是?
- Taper prednisone的時間有多長? 排除其他原因的 myopathy 排除light chain disease, 排除cancer ACE,排除Sarcoidosis
- The Lab data of this patient couldn`t help us much making diagnosis. We could only see that the kidney function dropping a little bit compared to the normal standard.It might belonged to the high age of the patient. While other data was noraml and the patient didn’t have
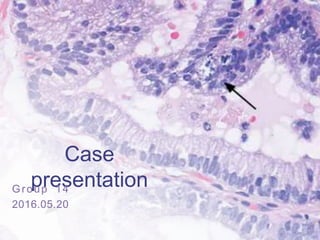
- A glandular mass (Panel A, arrows) appears underneath normal urothelium (arrowhead).
- high magnification (Panel B), neoplastic columnar cells form papillary (arrow) and tubular (arrowheads) structures. In addition to the ductal-type adenocarcinoma in the bladder neck, acinar-type prostatic adenocarcinoma (Panel C), Gleason score 6 (3+3), with a well-formed lumen (arrows) is seen in cores from the trans rectal biopsy of the prostate; the arrowhead shows a normal gland.
- According to the past history and biopsy,the tentative diagnosis was Urothelial carcinoma of the bladder neck, the prostatic urethra, or both.