Downloaded 10 times

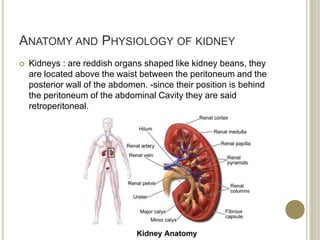
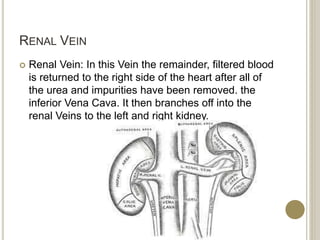
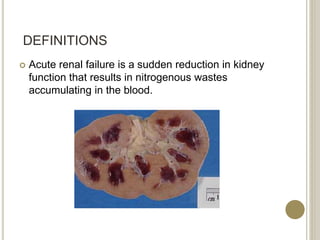
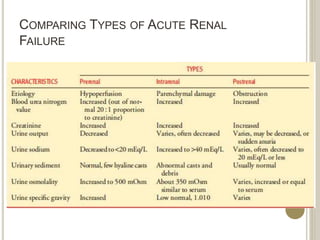
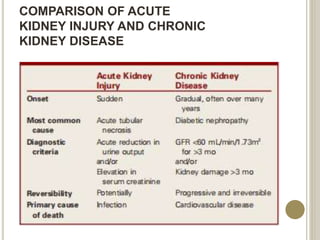


The document provides an overview of acute kidney failure, including its anatomy, physiology, causes, symptoms, diagnosis, treatment and complications. Some key points: - The kidneys are located in the back, protected by the ribs. They filter waste from the blood to produce urine. - Acute kidney failure is the sudden reduction of kidney function, causing waste to accumulate in the blood. It can be caused by dehydration, medications, infections and more. - Symptoms include reduced urine output, swelling, fatigue, shortness of breath and more. Diagnosis involves medical history, physical exam, blood and urine tests. - Treatment aims to correct fluid and electrolyte imbalances through IV fluids



































































