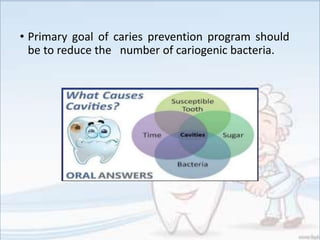
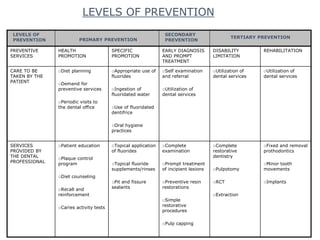
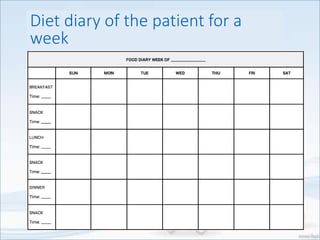
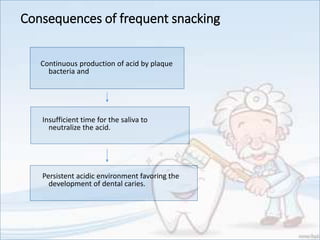
This document provides an overview of methods for preventing dental caries. It discusses the need for prevention due to issues like pain, compromised nutrition, and high treatment costs. The three levels of prevention - primary, secondary, and tertiary - are defined. Nutritional measures focus on diet analysis and counseling patients to reduce sugar intake and frequency of snacking. Chemical measures discuss the use of substances like fluoride, chlorhexidine, and probiotics to alter tooth surfaces or interfere with bacterial growth. Mechanical measures involve practices like toothbrushing and flossing.

























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












