Download to read offline



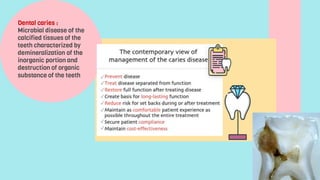

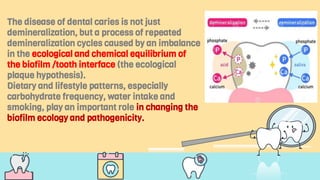
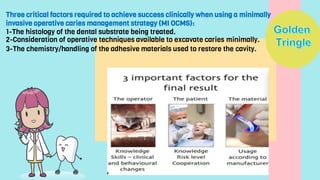
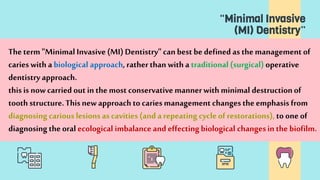
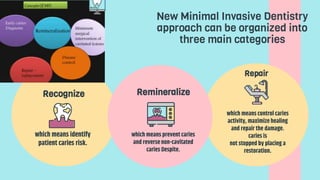



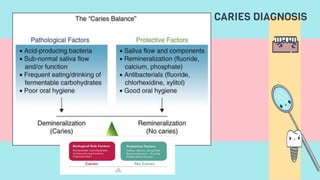
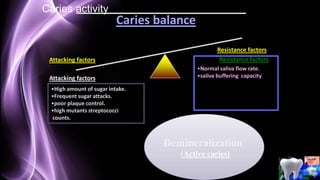
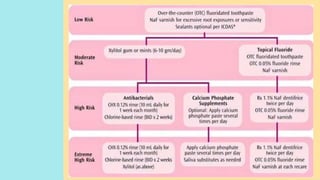
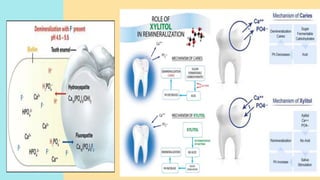
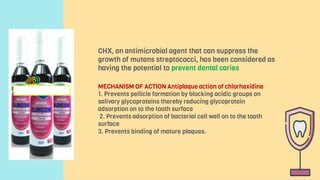
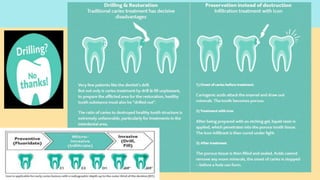



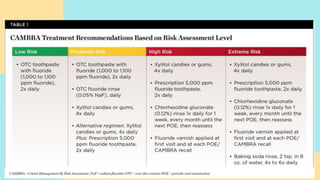
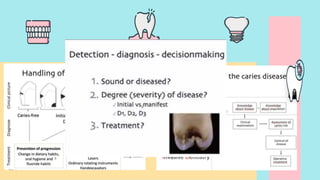
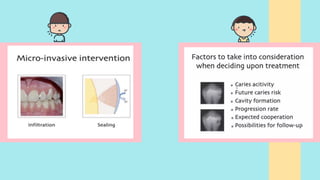
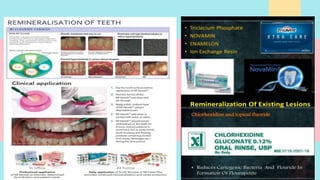
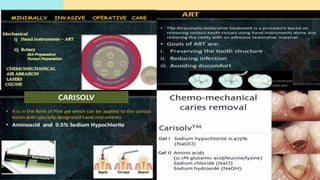

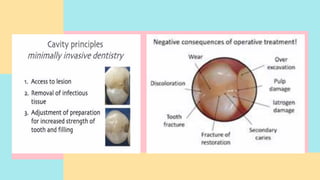
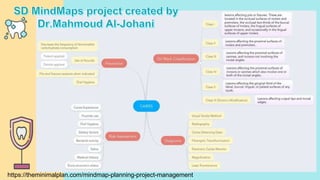
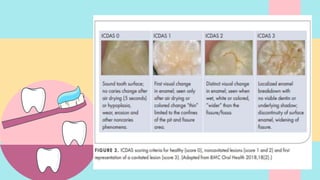


The document discusses the principles and techniques of minimal invasive dentistry for diagnosing and treating dental caries, including identifying patients' caries risk factors, using remineralization methods to prevent or control non-cavitated caries, and employing restorative techniques that minimize removal of healthy tooth structure. It outlines the goals of preserving tooth structure, stopping disease progression, and restoring function with minimal intervention. The approach focuses on changing the disease process through dietary and lifestyle modifications rather than solely operative treatment.




























![[1][m] minimally invasive restorative dentistry](https://cdn.slidesharecdn.com/ss_thumbnails/1mminimallyinvasiverestorativedentistry-160422162403-thumbnail.jpg?width=640&height=640&fit=bounds)


































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)
![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)