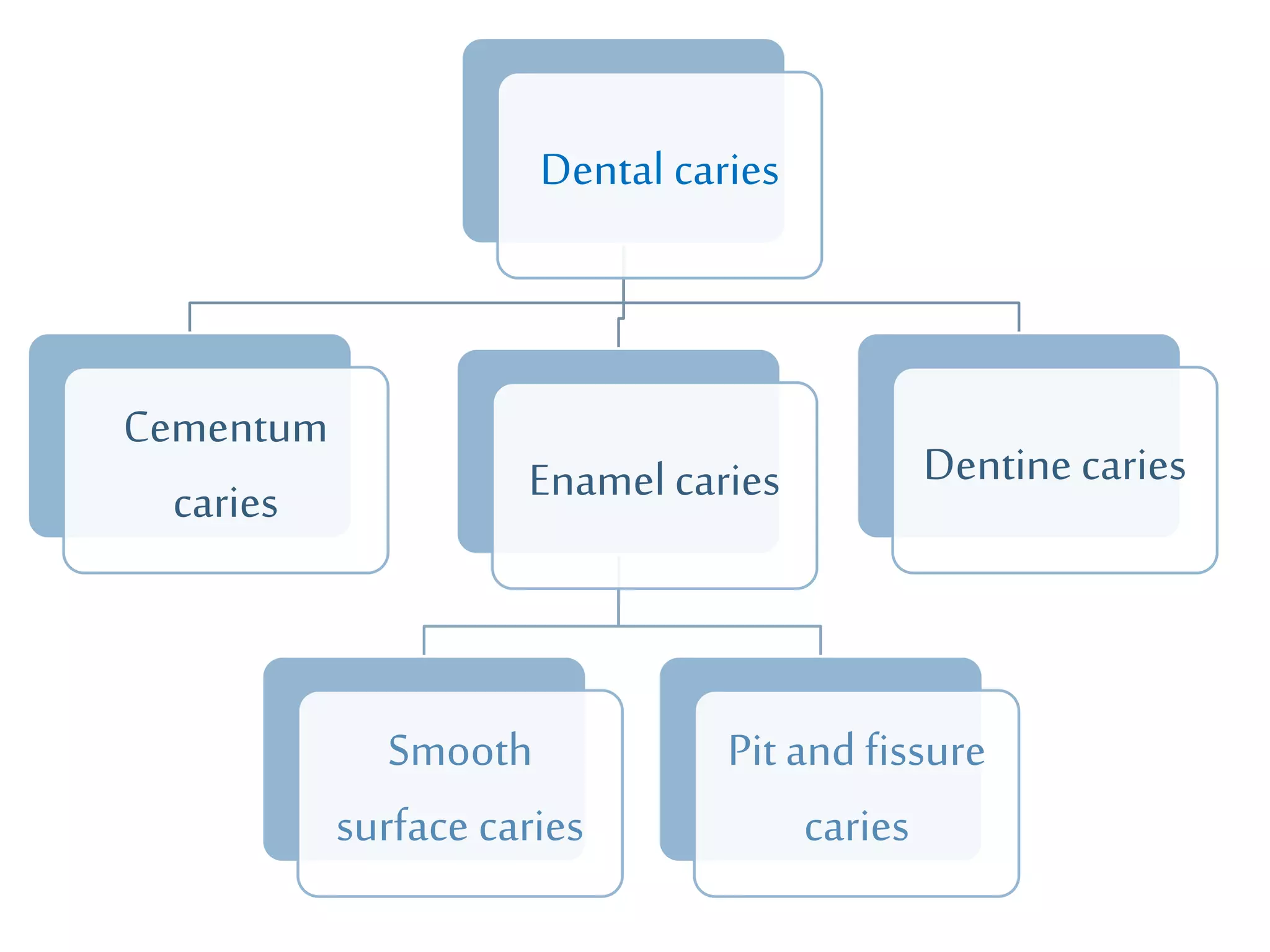
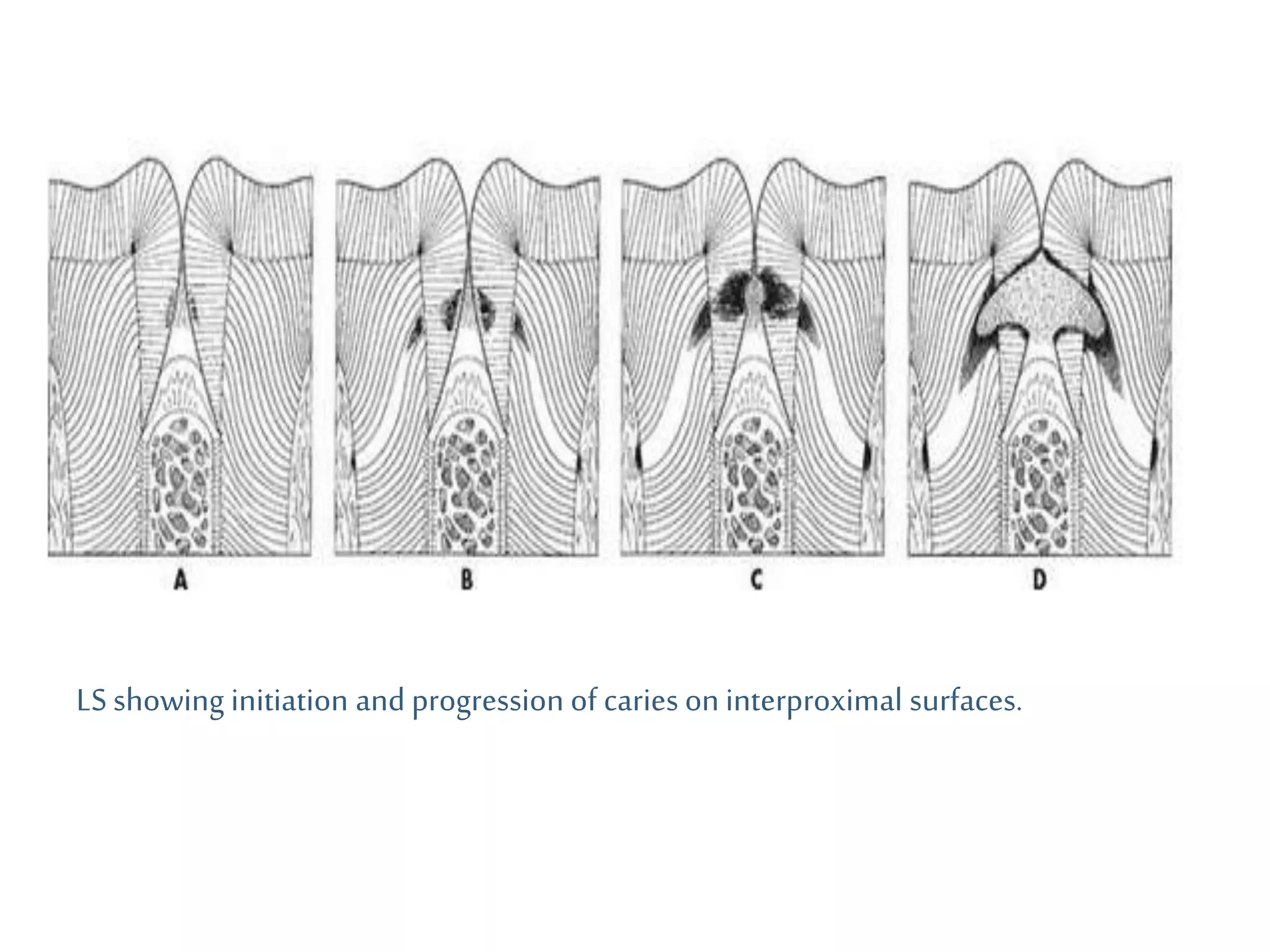
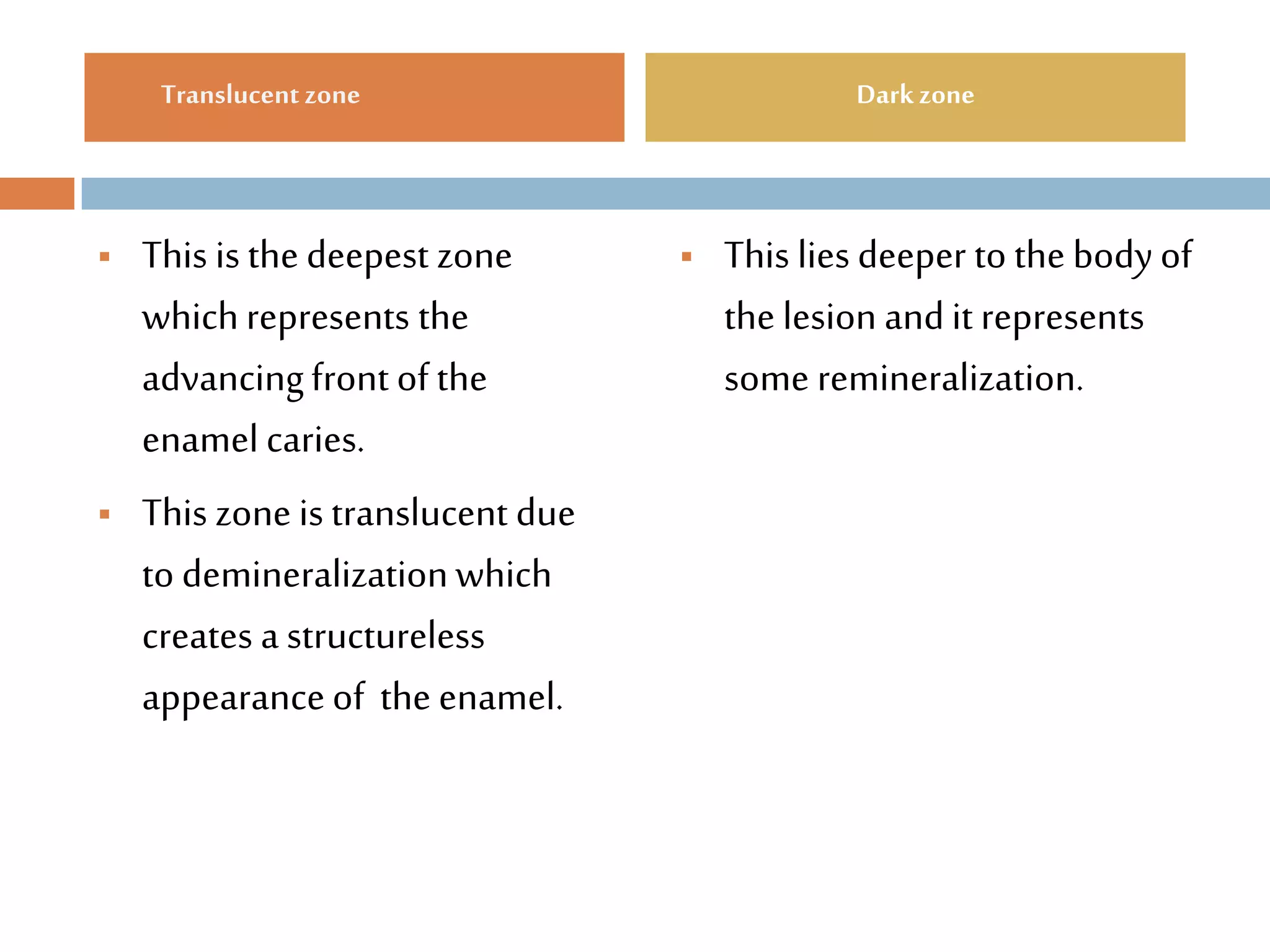
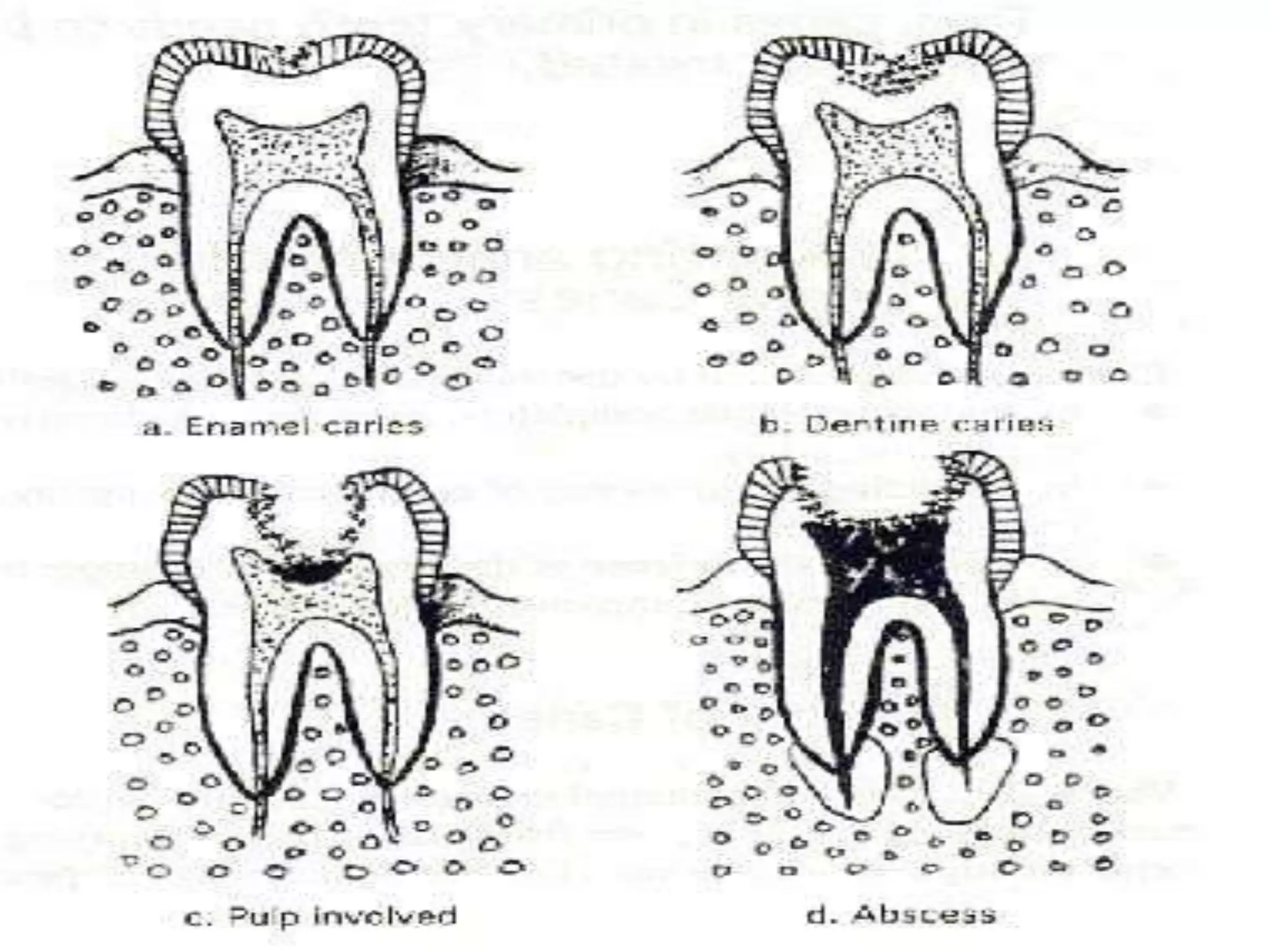
Dental caries is caused by bacteria in dental plaque that produce acids which demineralize tooth structure. The most common bacteria involved are Streptococcus mutans and Lactobacilli. There are several theories for how dental caries progresses, but it is now accepted that acids produced by bacteria lower the pH and cause the enamel and dentin to demineralize. Dental caries can affect the pits and fissures of teeth, smooth surfaces, or root surfaces. It is classified based on location, rate of progression, extent of damage, and other factors. Histologically, dental caries progresses through zones in enamel and dentin as the mineral content is reduced by acid attacks from bacteria.