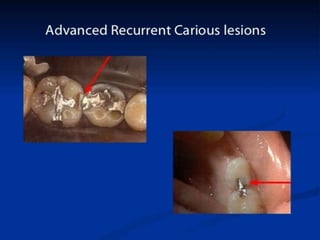
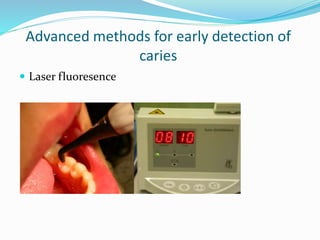
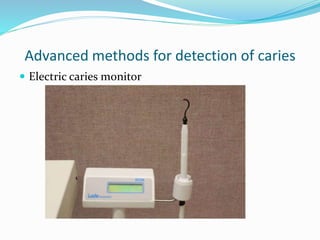
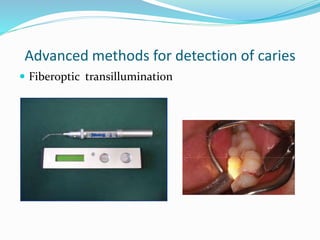
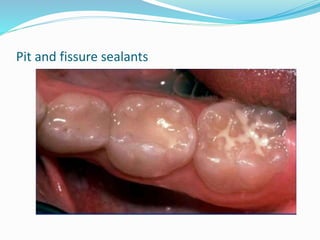
The document discusses the objectives and methods of caries diagnosis and prevention. It aims to identify lesions requiring treatment, persons at high risk, and assess factors like patient history, clinical examination, investigations. Prevention methods include plaque control, fluoride use, diet modification, pit and fissure sealants, and caries control restorations to limit bacterial growth and remineralize early lesions.




























![[Crown & Bridges] [terminology & classification]](https://cdn.slidesharecdn.com/ss_thumbnails/lec01-02terminologyclassification-151105130852-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)










![[1][m] minimally invasive restorative dentistry](https://cdn.slidesharecdn.com/ss_thumbnails/1mminimallyinvasiverestorativedentistry-160422162403-thumbnail.jpg?width=640&height=640&fit=bounds)