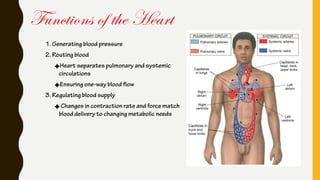
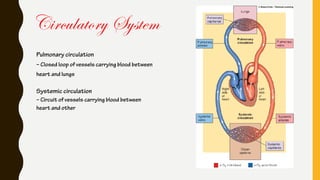
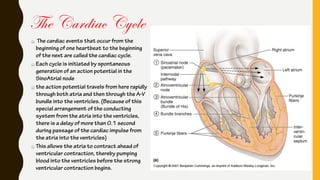
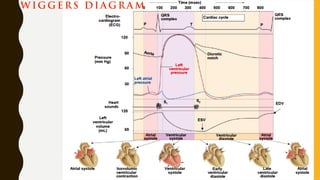
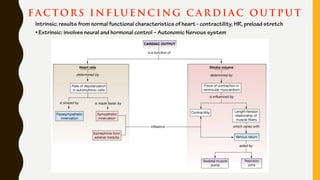
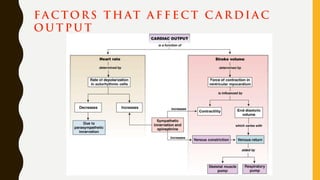
The heart functions to pump blood throughout the body via two circulatory systems - pulmonary and systemic. It generates blood pressure and ensures one-way blood flow. Cardiac output, the amount of blood pumped, is determined by heart rate and stroke volume. Intrinsic factors like the Frank-Starling mechanism and extrinsic neural and hormonal controls regulate cardiac output in response to the body's changing needs.








































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








