Downloaded 174 times






























This document discusses cardiac tamponade, including its anatomy, physiology, causes, clinical presentation, diagnosis and treatment. Cardiac tamponade is caused by an accumulation of fluid in the pericardial space that compresses the heart and impairs diastolic filling. It presents with symptoms like chest pain, dyspnea and pulsus paradoxus. Diagnosis is made through echocardiography, ECG changes and chest x-ray. Treatment involves drainage of pericardial fluid, usually through pericardiocentesis, along with medical management including oxygen, medications and ventilation.
Introduction to the topic of Cardiac Tamponade by Nurse Practitioner Pankaj Singh Rana from Swami Rama Himalayan University.
Discusses the pericardial anatomy, including the visceral and parietal layers, with fluid volumes in the pericardial space.
Explains the physiological role of the pericardium, its effects on cardiac chambers, and the concept of pericardial reserve volume.
Reviews how chronic pericardial stretching affects cardiac function and outlines its mechanical and immunological functions.
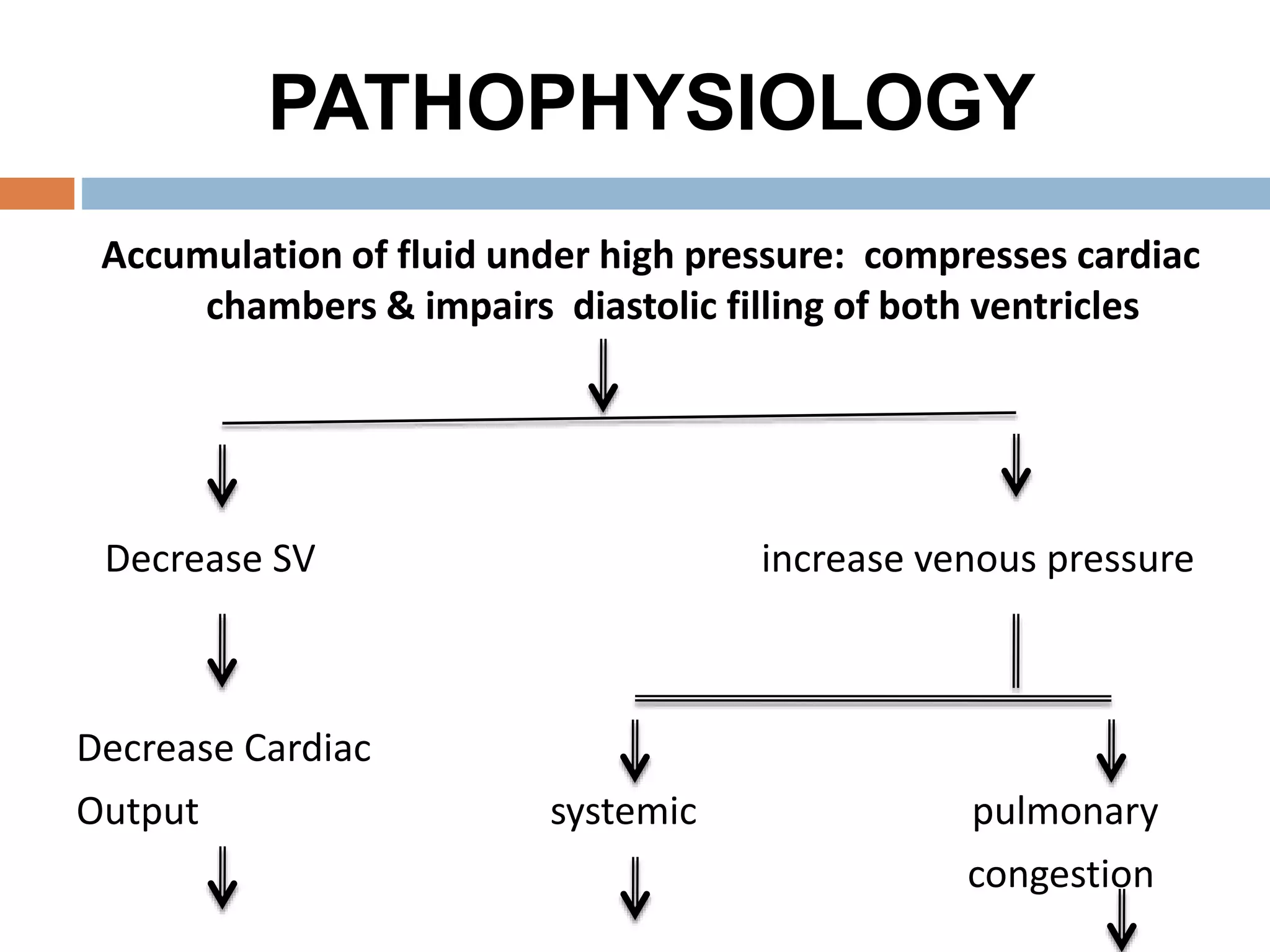
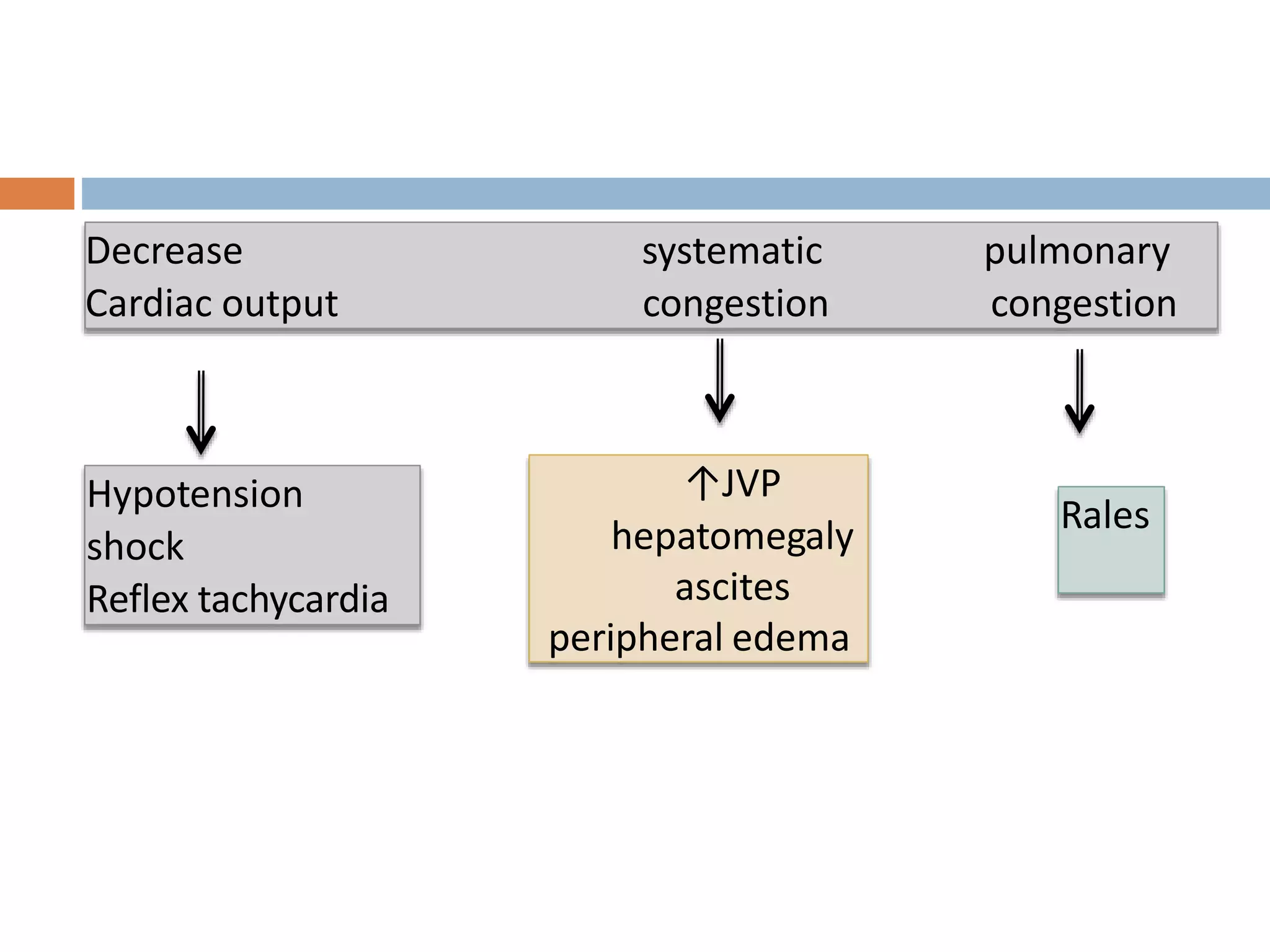
Describes the impact of fluid accumulation on cardiac chamber filling, leading to decreased cardiac output and signs of systemic congestion.
Outlines various causes of cardiac tamponade including idiopathic, infectious, and trauma-related factors.
Lists non-specific and specific symptoms associated with cardiac tamponade, including signs of distress and physical findings.
Defines pulsus paradoxus, its causes beyond cardiac tamponade, and how to measure it clinically.
Details significant physical exam findings and diagnostic methods, including JVP, ECG changes, and imaging techniques.Discusses both medical and surgical management strategies for resolving cardiac tamponade, emphasizing therapeutic interventions.
Concludes on the critical nature of cardiac tamponade, emphasizing diagnosis via echocardiography and pericardiocentesis as treatment.
Thanks the audience for their attention and concludes the presentation.























































































