Downloaded 1,331 times
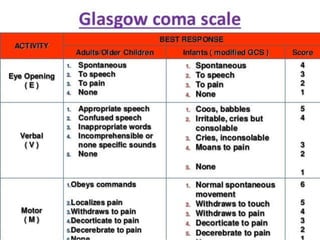
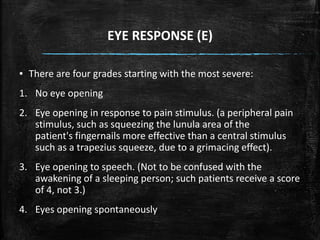
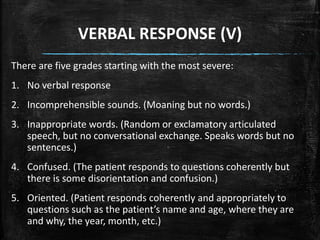
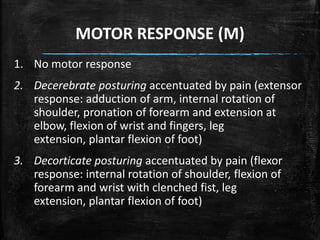
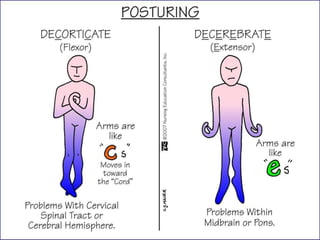
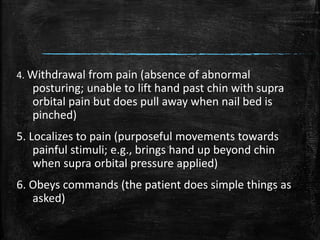
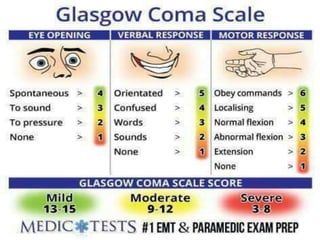
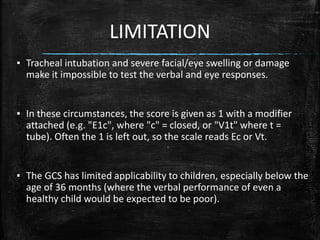



The Glasgow Coma Scale (GCS), developed in 1974, assesses a patient's consciousness through eye, verbal, and motor responses, scoring between 3 (deep unconsciousness) to 15 (full consciousness). It helps classify brain injuries as severe (GCS < 8-9), moderate (GCS 8-12), or minor (GCS ≥ 13), although limitations exist for cases involving tracheal intubation and young children. The documentation provides detailed scoring criteria for the three components and their interpretations.
































![glasgow coma scale gcs 2 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/gcs2autosaved-260117045741-a747a447-thumbnail.jpg?width=640&height=640&fit=bounds)






















































