NON INVASIVE TECHNIQUES
TRANSTHORACIC ECHO
BIO IMPEDENCE AND BIOREACTANCE
PULSE CONTOUR ANALYSIS
ULTRASOUND CARDIAC OUTPUT MONITOR
3.
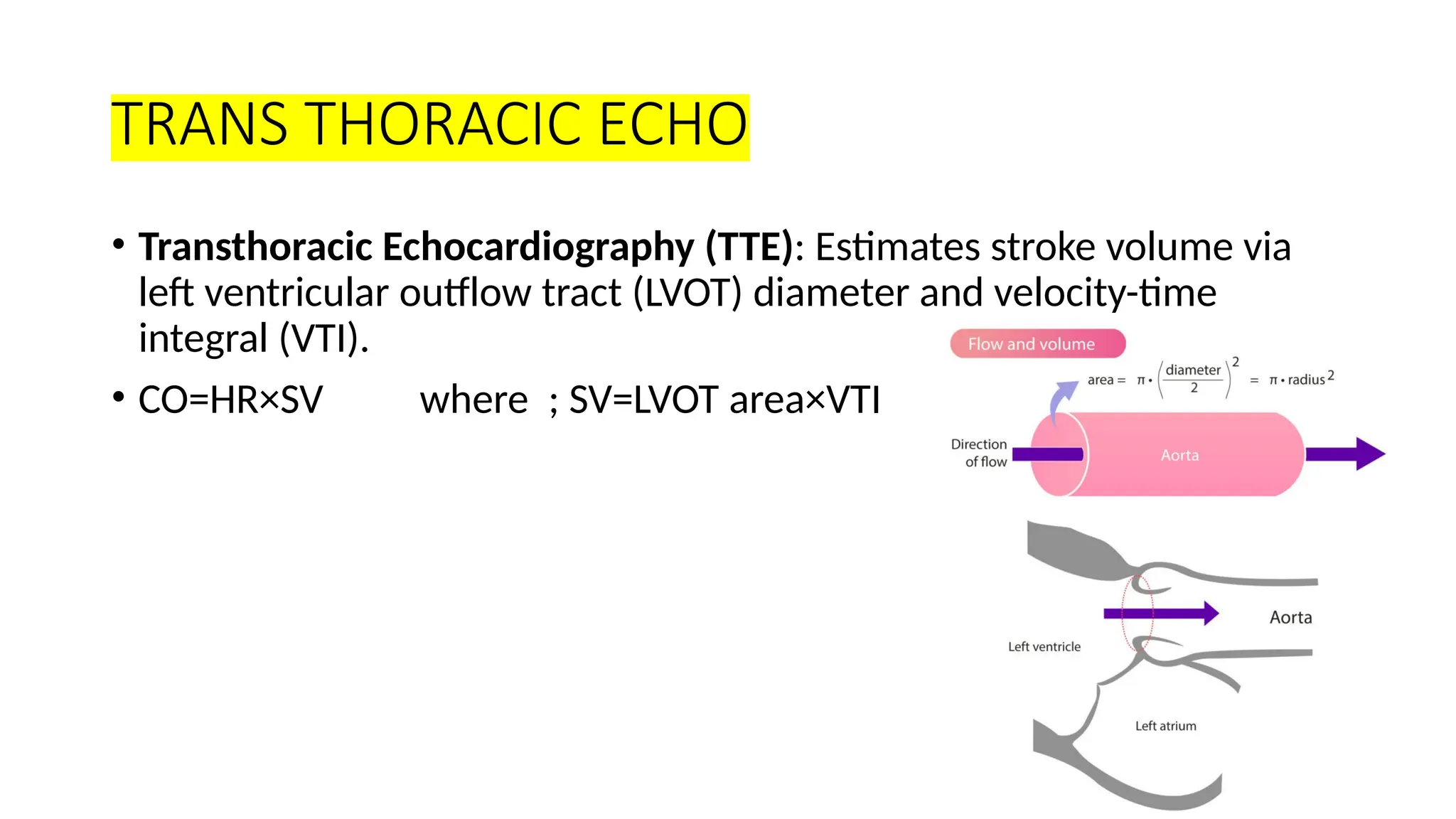
TRANS THORACIC ECHO
•Transthoracic Echocardiography (TTE): Estimates stroke volume via
left ventricular outflow tract (LVOT) diameter and velocity-time
integral (VTI).
• CO=HR×SV where ; SV=LVOT area×VTI
4.
• VTI (VelocityTime Integral) is the distance a column of blood travels
during one heartbeat, calculated from the Doppler waveform
• It’s essentially the area under the curve of a Doppler velocity vs. time
graph.
• The cursor is placed at a specific valve (most commonly the left
ventricular outflow tract – LVOT) to record the blood flow velocity
over time.
5.
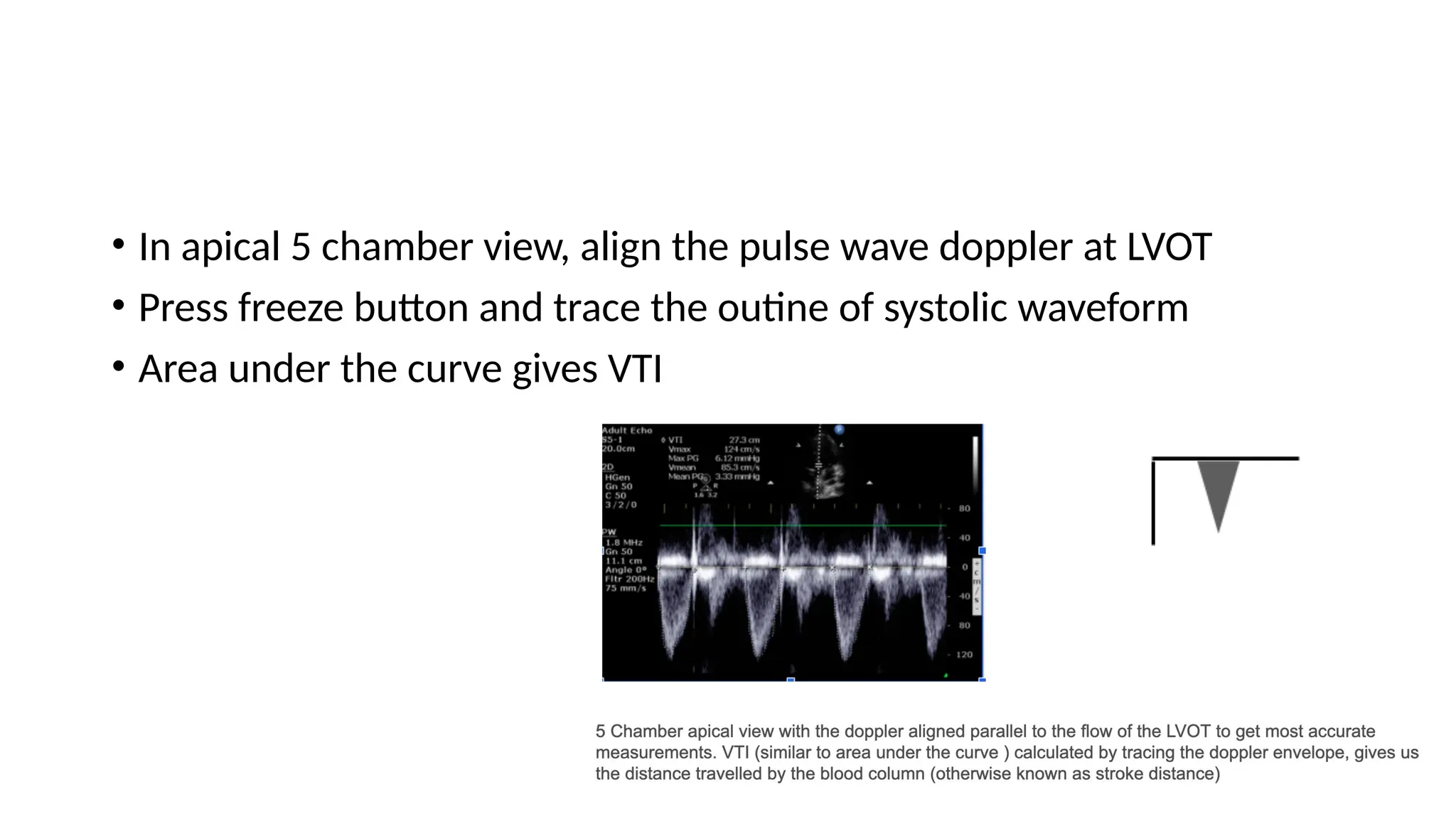
• In apical5 chamber view, align the pulse wave doppler at LVOT
• Press freeze button and trace the outine of systolic waveform
• Area under the curve gives VTI
6.
BIO IMPEDENCE ANDBIO REACTANCE
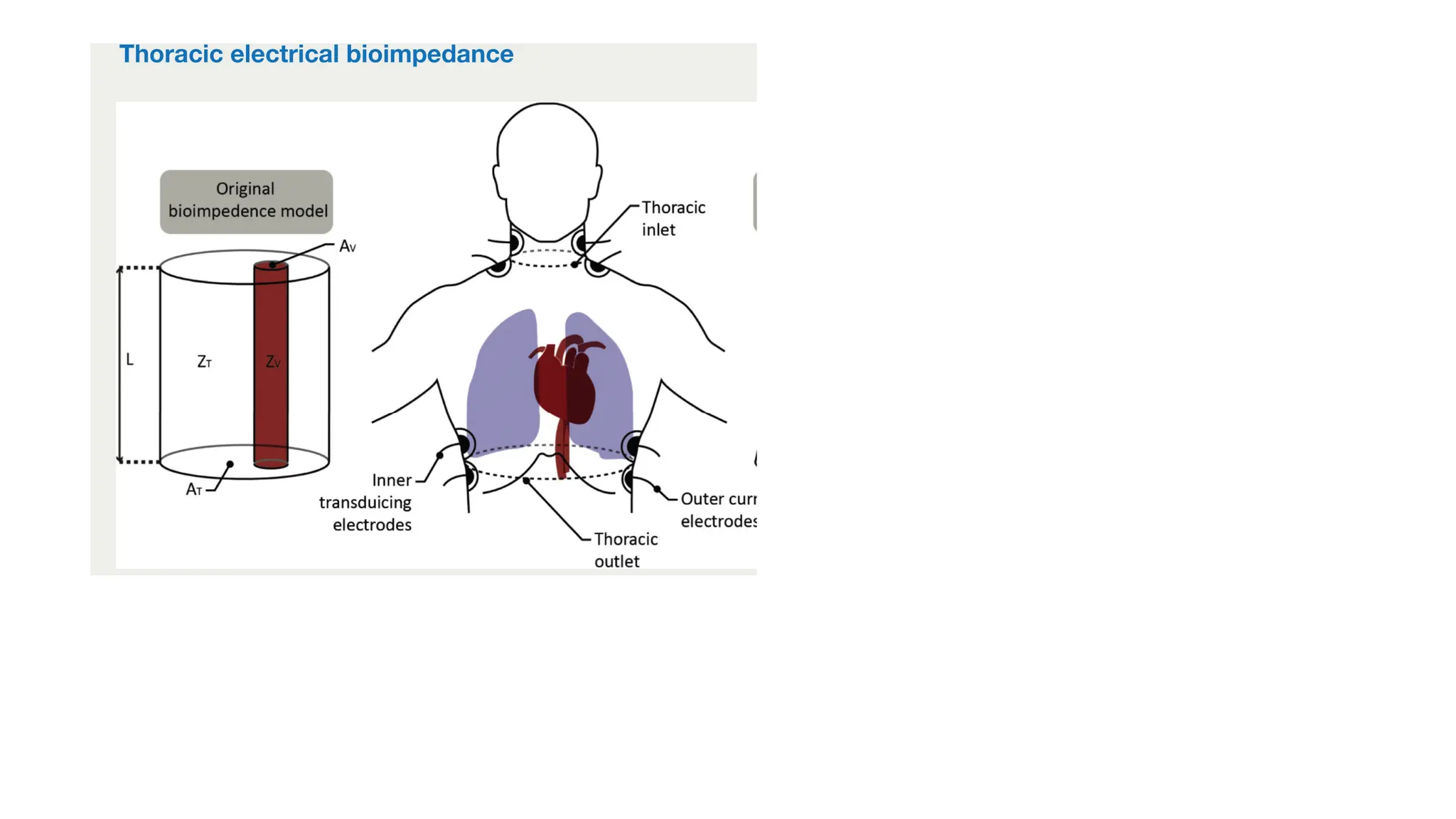
• Measures changes in thoracic impedance(resistance) related to blood
flow.
• 6 Electrodes are placed on the skin (neck, chest, or torso)
• A small electrical current is passed through the thorax.
• As the heart pumps, the volume of blood in the thoracic aorta
changes, altering the resistance to current (impedance).
• These changes are used to estimate stroke volume and cardiac
output.
8.
Bio reactance
• Sameelectrode setup as bioimpedance
• Instead of measuring resistance (magnitude), it tracks phase shifts
(timing of the current signal) caused by pulsatile blood flow
• It measures the change in voltage signal applied across the thorax
9.
PULSE CONTOUR ANALYSIS
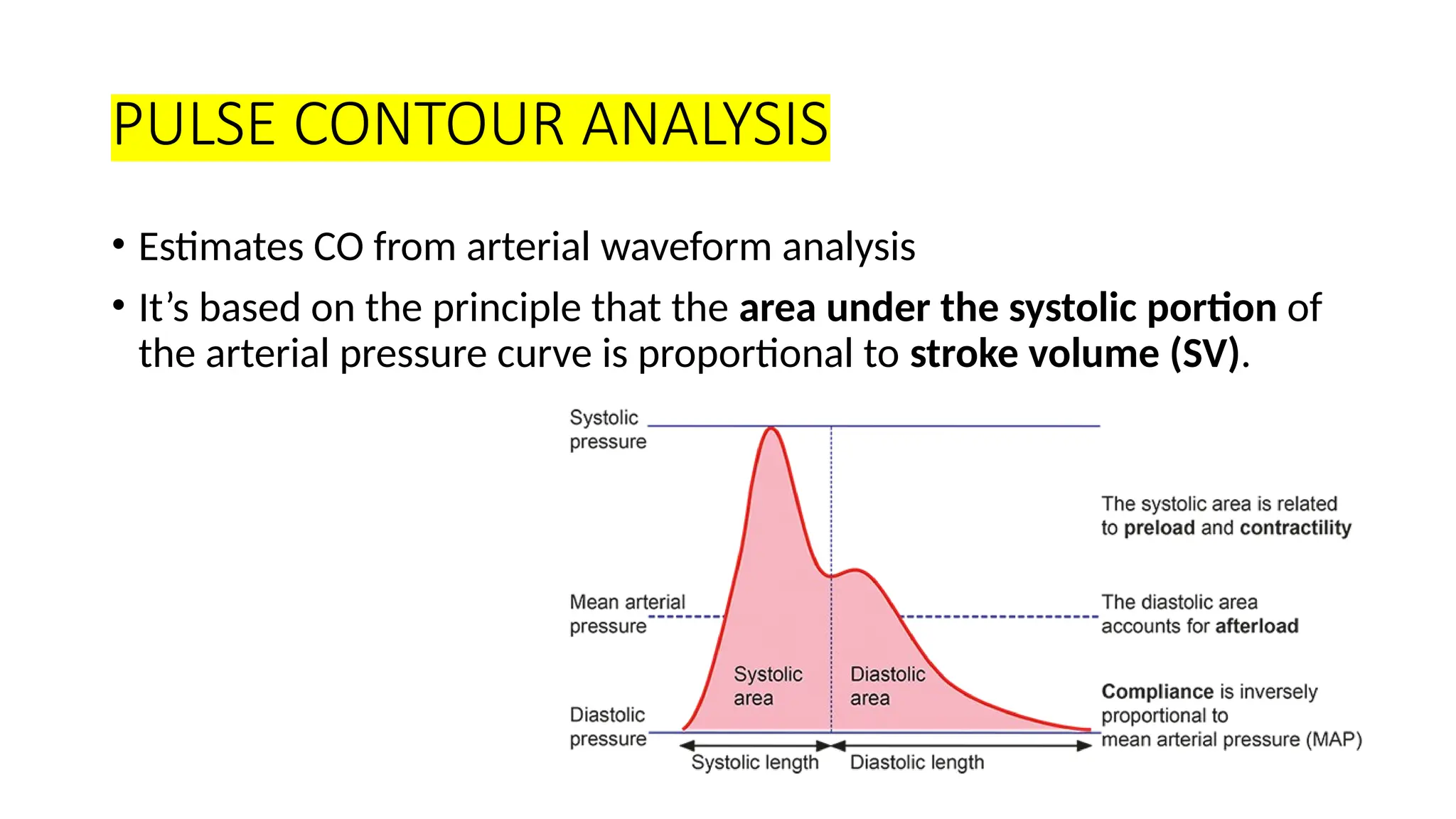
•Estimates CO from arterial waveform analysis
• It’s based on the principle that the area under the systolic portion of
the arterial pressure curve is proportional to stroke volume (SV).
10.
• Arterial waveformis obtained via an invasive arterial line (like radial
or femoral)
• The shape of the pressure wave is analyzed beat by beat.
11.
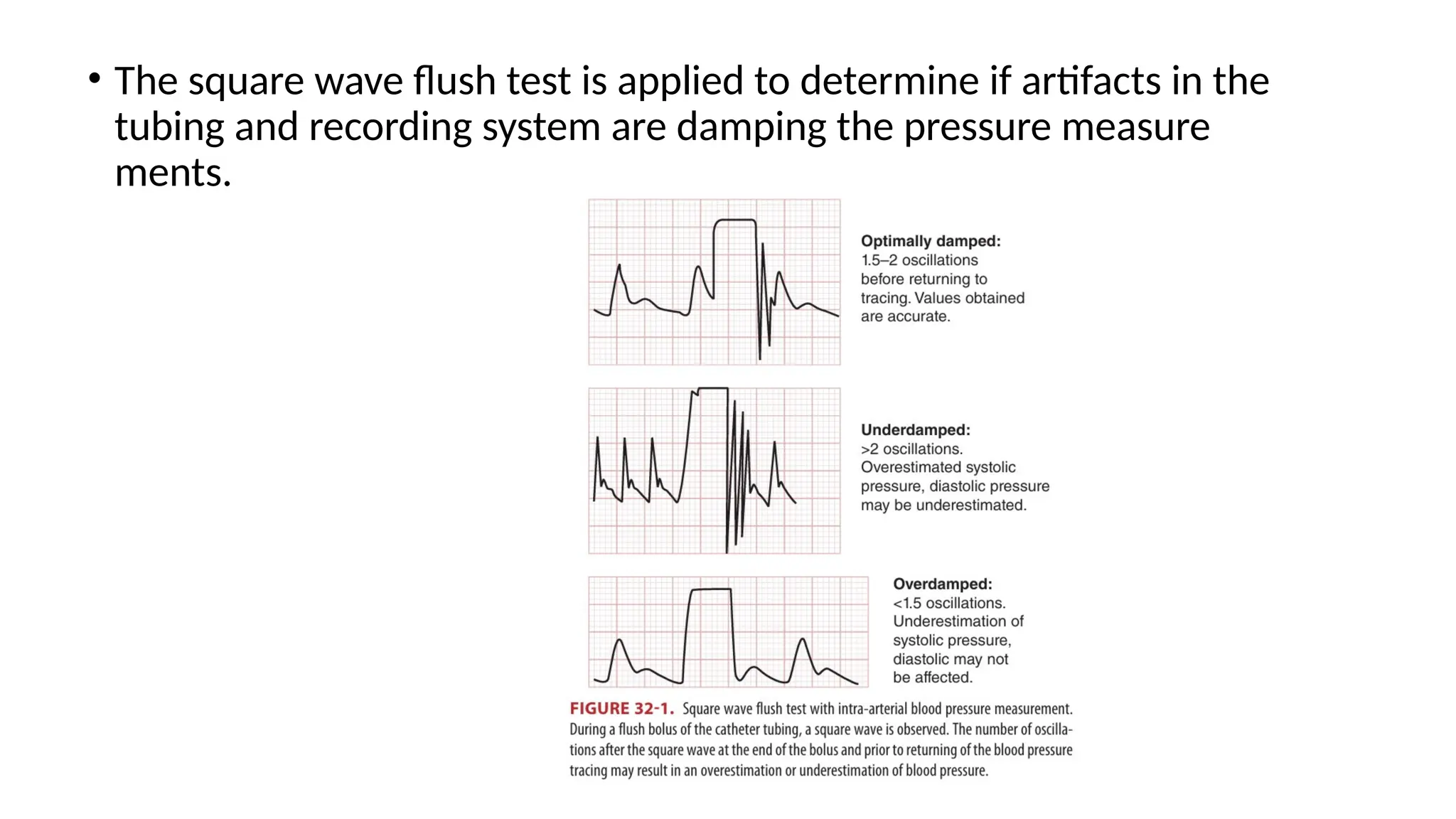
• The squarewave flush test is applied to determine if artifacts in the
tubing and recording system are damping the pressure measure
ments.
12.
ULTRASOUND CARDIAC OUTPUTMONITRING
• It’s a non-invasive Doppler-based device used for real-time
assessment of cardiac output and hemodynamics at the bedside
• It provides:
• Cardiac Output (CO)
• Stroke Volume (SV)
• Systemic Vascular Resistance (SVR)
• Flow time, heart rate, and volume responsiveness
13.
• Patient Setup-Supine or semi-recumbent position
• Aortic view: Place probe at suprasternal notch, aiming caudally
toward the aortic arch
• Pulmonary view: Place probe at left parasternal 2nd–3rd ICS, angled
toward right ventricular outflow tract
• Adjust transducer to get clean waveform
• Record 3–5 clean waveforms
• USCOM automatically averages and calculates hemodynamic
parameters
PULMONARY ARTERY CATHETERISATION
•Pulmonary Artery Catheterization (PAC) is an invasive hemodynamic
monitoring technique that involves inserting a catheter into the right
side of the heart and into the pulmonary artery
• It allows direct measurement of pressures, cardiac output, and
oxygen delivery parameters.
16.
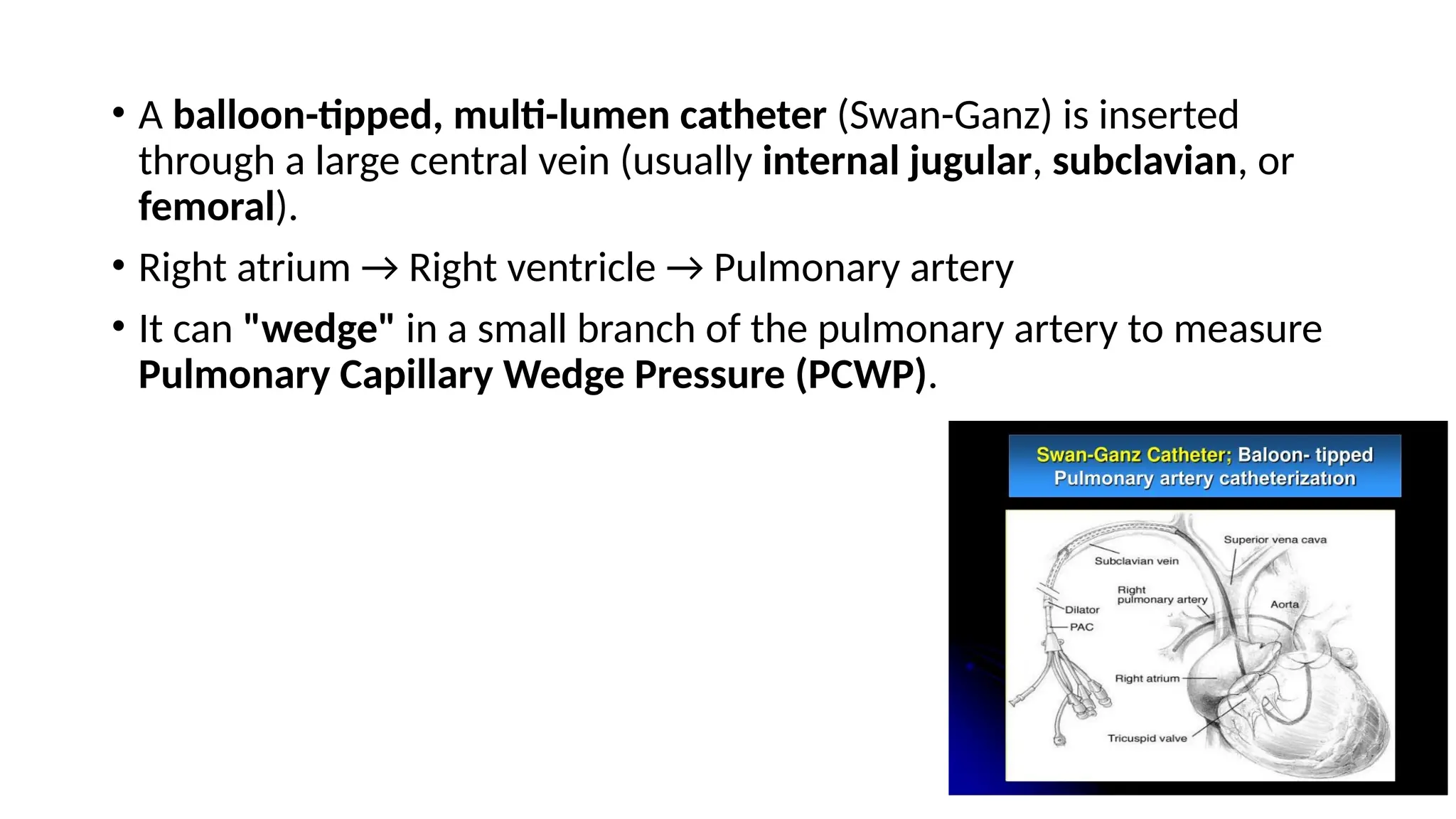
• A balloon-tipped,multi-lumen catheter (Swan-Ganz) is inserted
through a large central vein (usually internal jugular, subclavian, or
femoral).
• Right atrium → Right ventricle → Pulmonary artery
• It can "wedge" in a small branch of the pulmonary artery to measure
Pulmonary Capillary Wedge Pressure (PCWP).
17.
THERMODILUTION
• Thermodilution isa method of calculating cardiac output by
measuring how a known temperature change (caused by injecting
cold fluid) affects blood temperature downstream.
18.
• A knownvolume (usually 5–10 mL) of cold saline (room temp or iced)
is rapidly injected into the right atrium via the proximal port of the
PAC.
• The cold saline mixes with the blood as it travels through the right
ventricle → pulmonary artery.
• A thermistor near the catheter tip in the pulmonary artery measures
the change in blood temperature over time.
19.
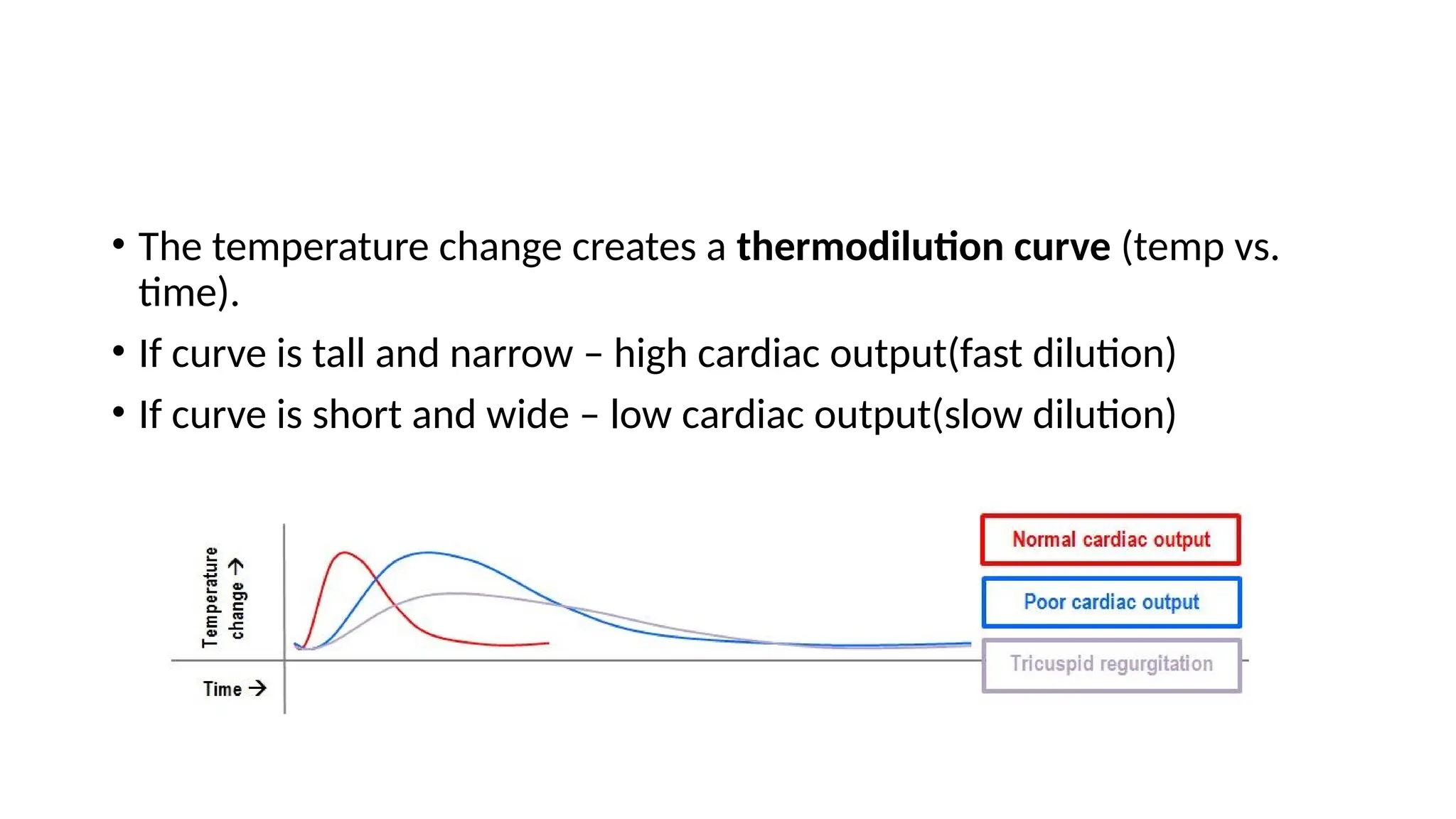
• The temperaturechange creates a thermodilution curve (temp vs.
time).
• If curve is tall and narrow – high cardiac output(fast dilution)
• If curve is short and wide – low cardiac output(slow dilution)
20.
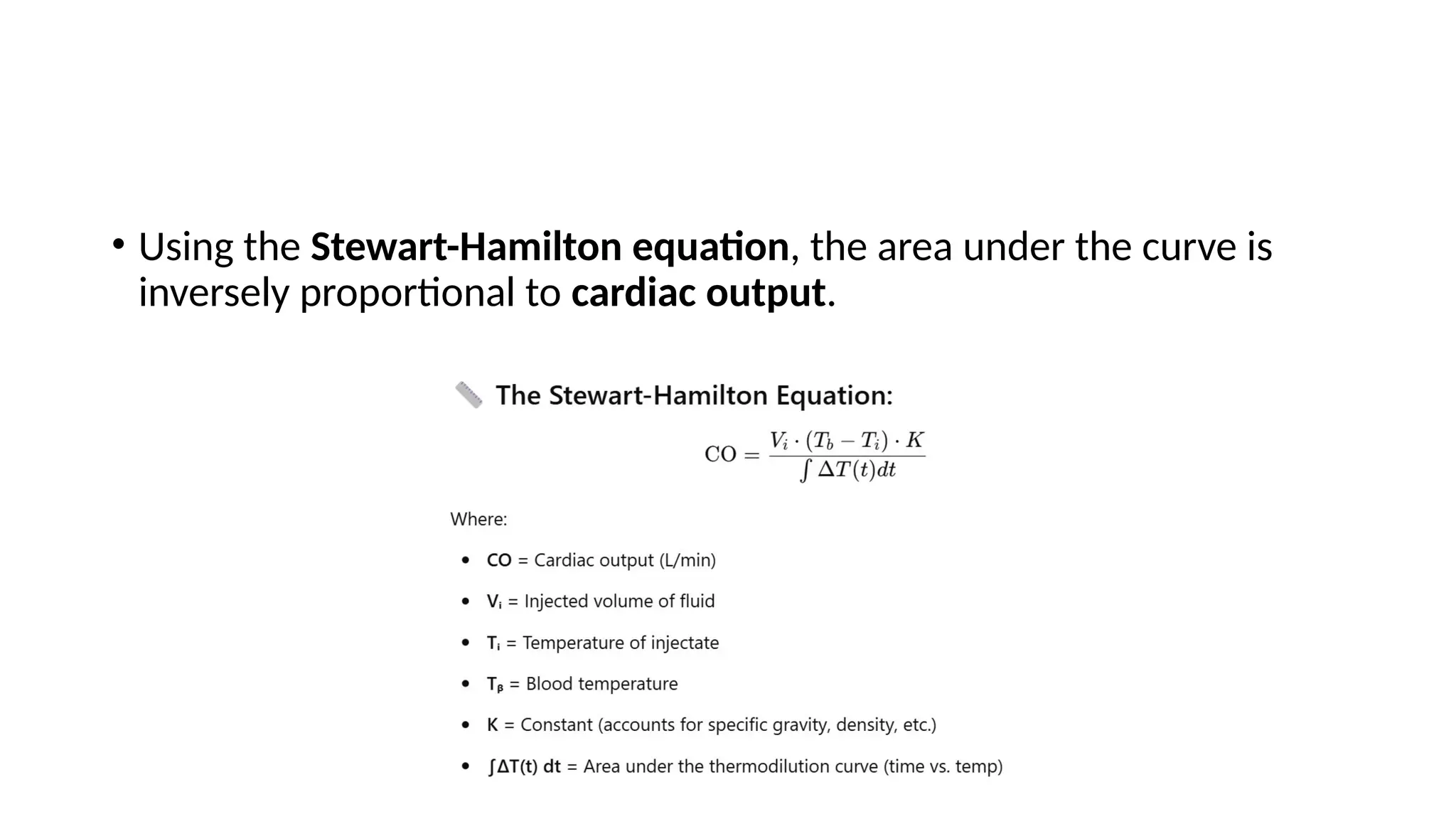
• Using theStewart-Hamilton equation, the area under the curve is
inversely proportional to cardiac output.
21.
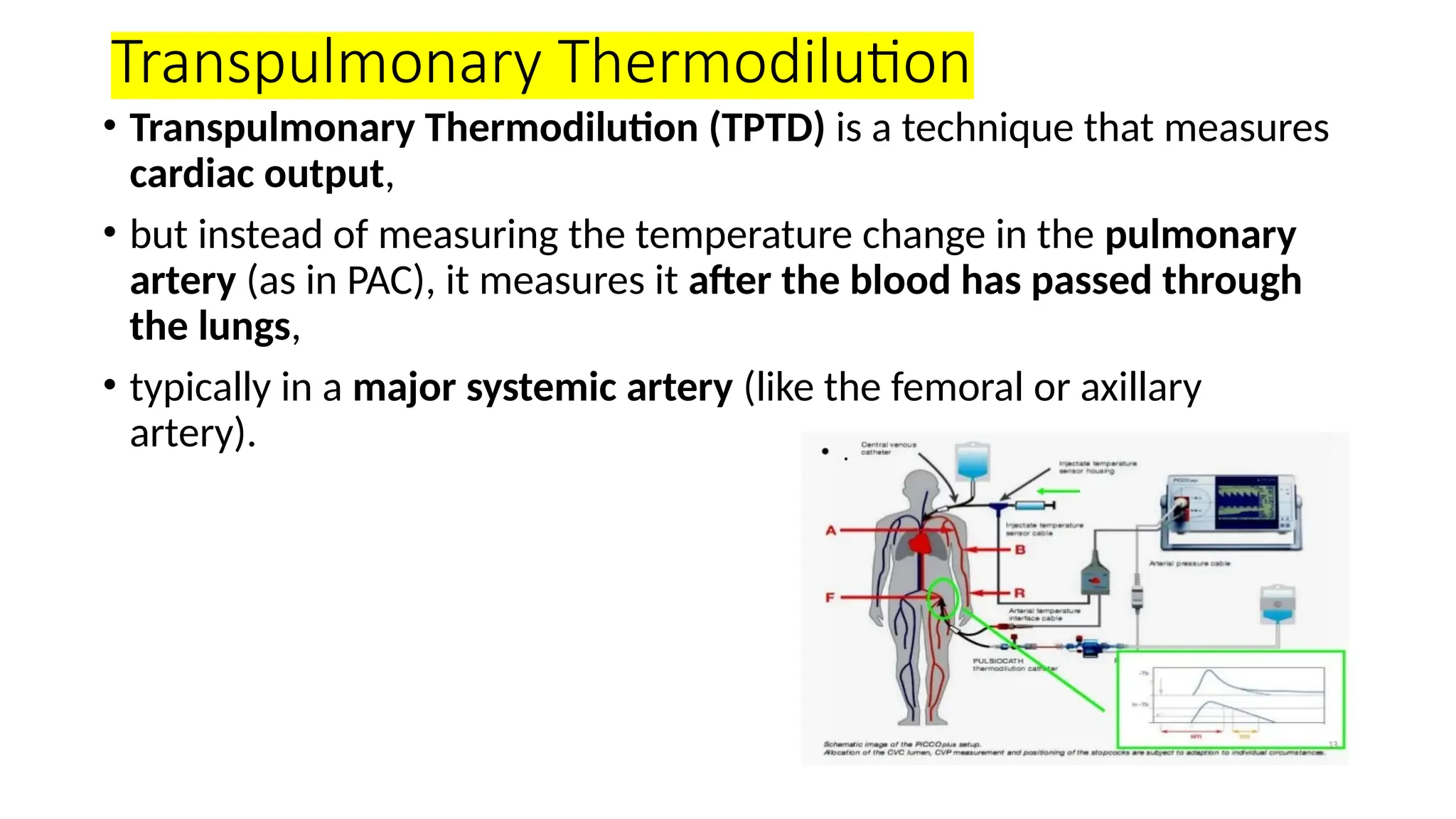
Transpulmonary Thermodilution
• TranspulmonaryThermodilution (TPTD) is a technique that measures
cardiac output,
• but instead of measuring the temperature change in the pulmonary
artery (as in PAC), it measures it after the blood has passed through
the lungs,
• typically in a major systemic artery (like the femoral or axillary
artery).
22.
• A coldsaline bolus (usually 15–20 mL) is injected into a central
venous catheter (usually via a jugular or subclavian vein).
• Right heart → pulmonary circulation → left heart → systemic
circulation
• A thermistor-tipped arterial catheter (usually femoral or axillary)
detects the temperature change.
• Cardiac output (CO) is calculated using the modified Stewart-
Hamilton equation—similar to PAC thermodilution

























![Clinicalteaching [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/clinicalteachingautosaved-180718063103-thumbnail.jpg?width=640&height=640&fit=bounds)






















