Download to read offline







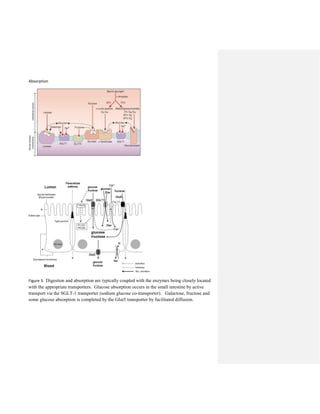

Carbohydrates are a significant energy source in the diet, primarily providing glucose through digestion in the small intestine where they are broken down into monosaccharides. The digestion process begins in the mouth with salivary amylase, but further breakdown occurs in the small intestine through pancreatic amylase and brush border enzymes. Absorption of glucose and galactose is facilitated by the sglt-1 transporter, while fructose is absorbed via the glut5 transporter, with various factors influencing the efficiency of absorption and potential disorders such as lactose intolerance or disaccharidase deficiencies impacting carbohydrate digestion.






































































