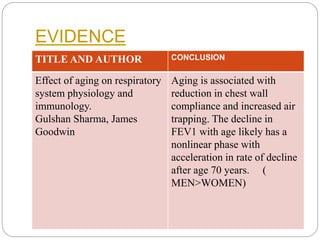
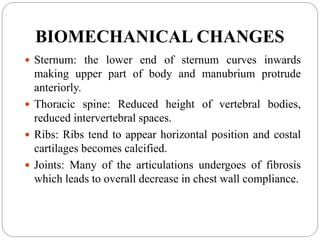
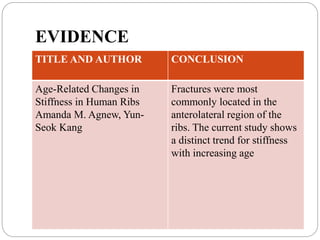
This document provides a review of literature on age-related cardiopulmonary changes. It summarizes research showing that aging leads to structural and functional changes in both the cardiovascular and respiratory systems. For the cardiovascular system, changes include increased stiffness of arteries and valves, decreased compliance of heart walls, and alterations in the electrical conduction system. For the respiratory system, aging causes a loss of elastic recoil in the lungs, decreased compliance of the chest wall and ventilatory muscles, and a decline in both diffusion capacity and maximal aerobic power. The integration of cardiovascular and pulmonary systems during exercise is also impacted by aging.









![Physiotherapy in pulmonary_surgery[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonarysurgery1-230705093621-2b78f958-thumbnail.jpg?width=640&height=640&fit=bounds)













































![ergonomics[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ergonomics1-230226092320-24f170c5-thumbnail.jpg?width=640&height=640&fit=bounds)



























