Downloaded 19 times




![Anticoagulation therapy
1. Low-molecular-weight heparin (e.g. Enoxaparin
[Lovenox])
2. Unfractionated heparin, or one of the new oral
anticoagulants (NOACs), such as a direct thrombin
inhibitor (e.g., dabigatran [Pradaxal]) or a Factor Xa
inhibitor (e.g., fondaparinux [Arixtral], rivaroxaban
[Xarelto], apixaban [Eliquis], or edoxaban [Savaysa]
3. Warfarin (Coumadin)](https://image.slidesharecdn.com/acutepulmonaryembolism-210610133306/85/Acute-pulmonary-embolism-and-its-management-52-320.jpg)




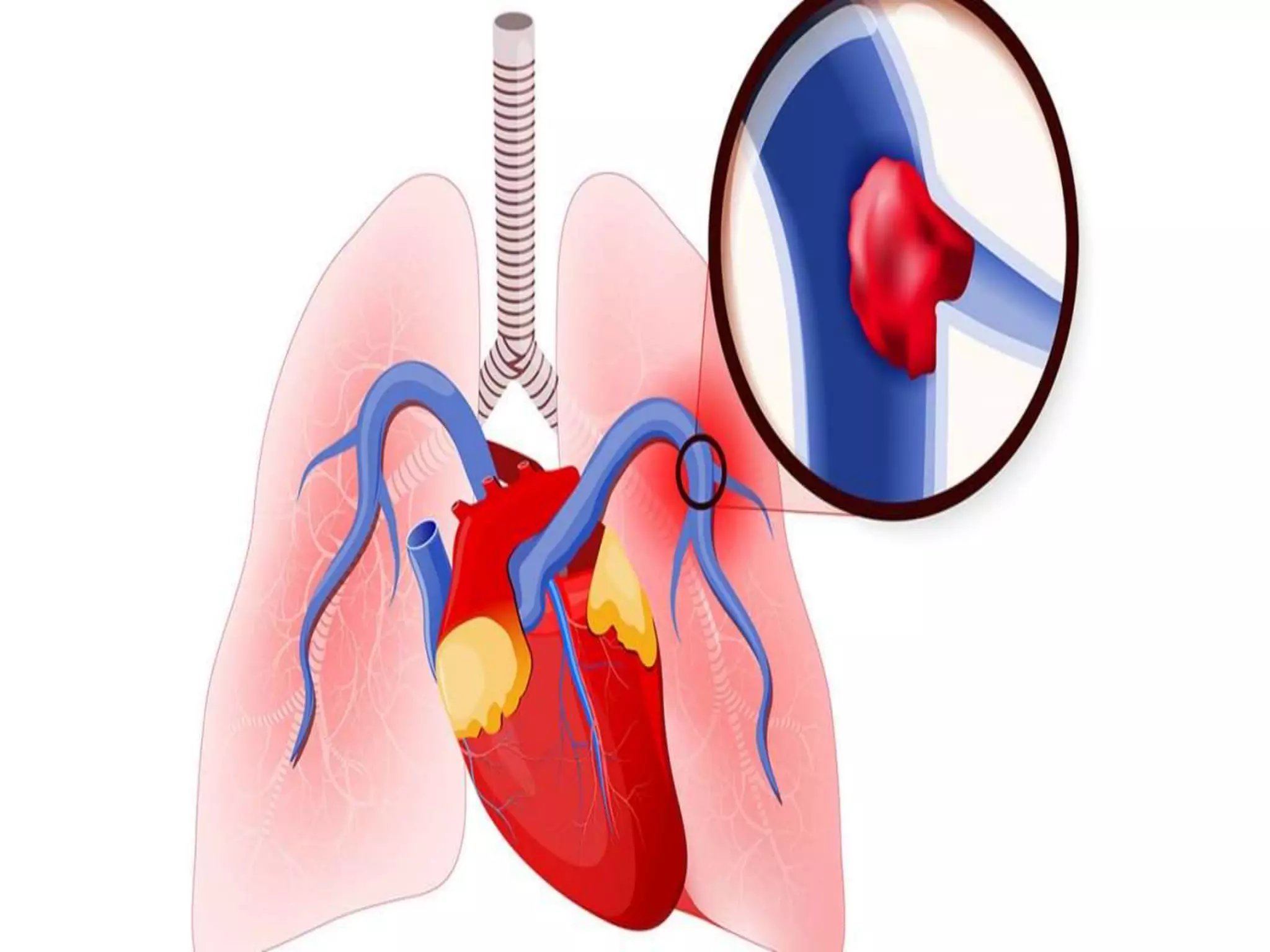
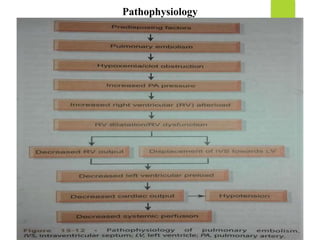
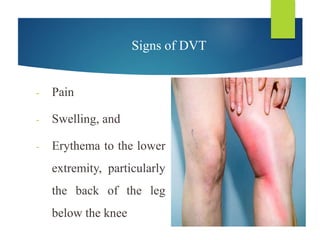
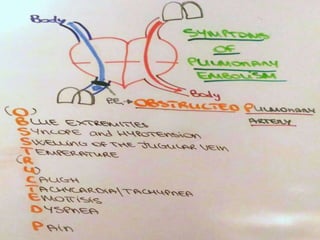
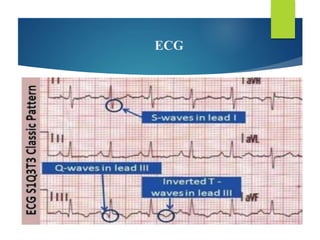
Acute pulmonary embolism is a life-threatening condition caused by the obstruction of pulmonary arteries due to blood clots or other materials. The document outlines its epidemiology, clinical features, risk factors, diagnostic methods, management strategies, and nursing care. Emphasis is placed on prevention and the urgent need for emergency treatment to stabilize the patient.