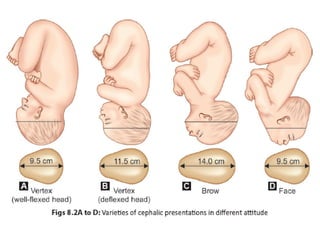
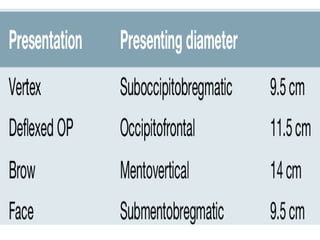
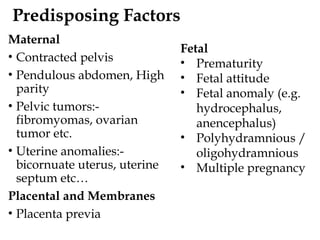
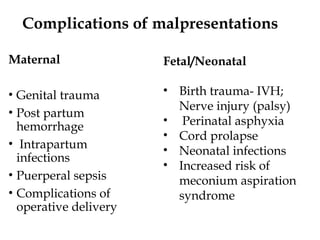
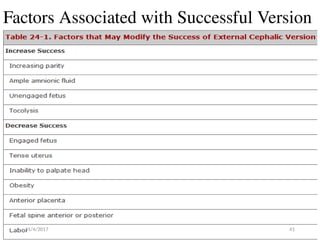
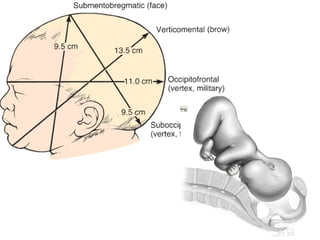
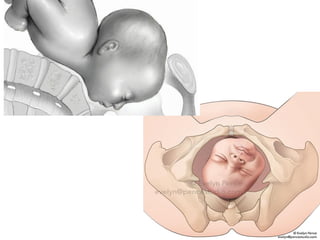
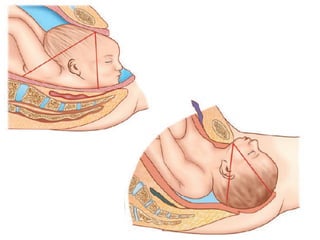
The document discusses malpresentations in childbirth, defining various types such as breech, face, brow, and shoulder presentations, as well as their complications for both mother and fetus. It outlines diagnostic methods, management strategies including vaginal delivery and cesarean options, and factors influencing the likelihood of these presentations. Additionally, it provides details about potential risks and complications associated with each type of malpresentation during labor and delivery.

























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


