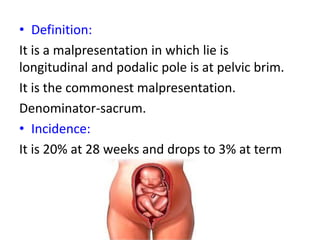
This document discusses breech presentation during childbirth. It defines breech presentation and notes its incidence decreases with gestational age. Complications for mother and baby from breech delivery are described. The document classifies breech presentations and reviews etiology, diagnosis, labor mechanism, and management approaches including external cephalic version, vaginal delivery, and cesarean section. Specific techniques for assisting various stages of vaginal breech delivery are outlined. Factors influencing management decisions are also summarized.