Downloaded 141 times
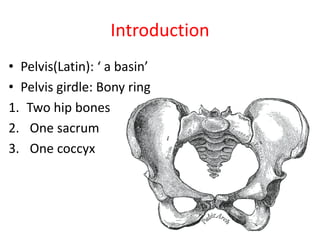

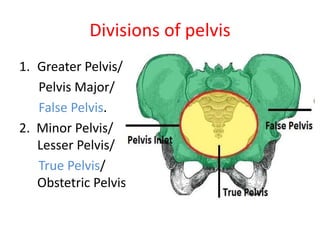
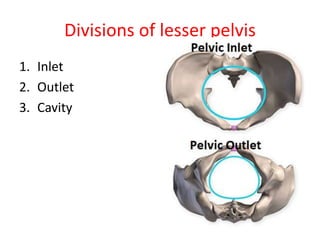
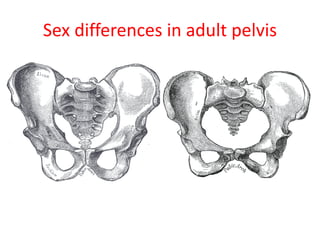
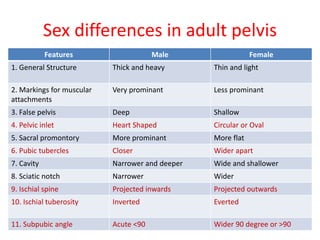
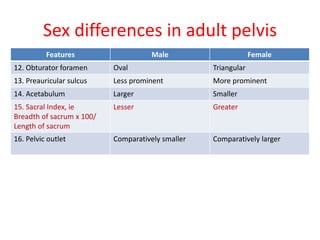



The document provides an overview of the bony pelvis, including its functions, divisions, boundaries, diameters, sex differences, and applied anatomy. Key points include: - The pelvis is composed of bones including the two hip bones, sacrum, and coccyx. It functions in locomotion, weight transmission, muscle attachments, and protection of pelvic organs. - The pelvis is divided into the greater pelvis and lesser pelvis (true pelvis), with the latter further divided into the inlet, outlet, and cavity. - Sex differences in the adult pelvis include a thicker and heavier structure in males versus thinner and lighter in females. Dimensions like the subpubic angle and























































































