Downloaded 18 times

![ It is made up of 4 bones
1. Os innominatum [2]
2. Sacrum
3. Coccyx
Os innominatum is made up of 3 bones
1. Ilium
2. Ischium
3. Pubis](https://image.slidesharecdn.com/pelvis-200323054350/75/Pelvis-Obstetrical-Significance-2-2048.jpg)
![ Pelvis has 4 joints
1. Pubic symphysis – Fibrocartilagenous jt. It
has 3 ligaments – superior and inferior pubic
ligaments and arcuate ligament in between
2. Sacroiliac jt. Or synchondrosis [2] -
synovial
3. Sacrococcygeal jt. – Synovial hinge](https://image.slidesharecdn.com/pelvis-200323054350/75/Pelvis-Obstetrical-Significance-3-2048.jpg)
![ 1. Angle of inclination – 55-60 degrees [more
the angle bad is outcome]
2. Sacral Angle – 90 degrees [ less is bad]
3. Subpubic angle – 85-90 degrees [ less is
bad and it will increase waste space of
Morris]](https://image.slidesharecdn.com/pelvis-200323054350/75/Pelvis-Obstetrical-Significance-4-2048.jpg)


![ There are 4 types – Caldwell Moloy
classification
1. Gynaecoid type [50%]
2. Android type [25 %]
3. Anthropoid type [20%]
4. Platypelloid type [ 5%]](https://image.slidesharecdn.com/pelvis-200323054350/75/Pelvis-Obstetrical-Significance-8-2048.jpg)
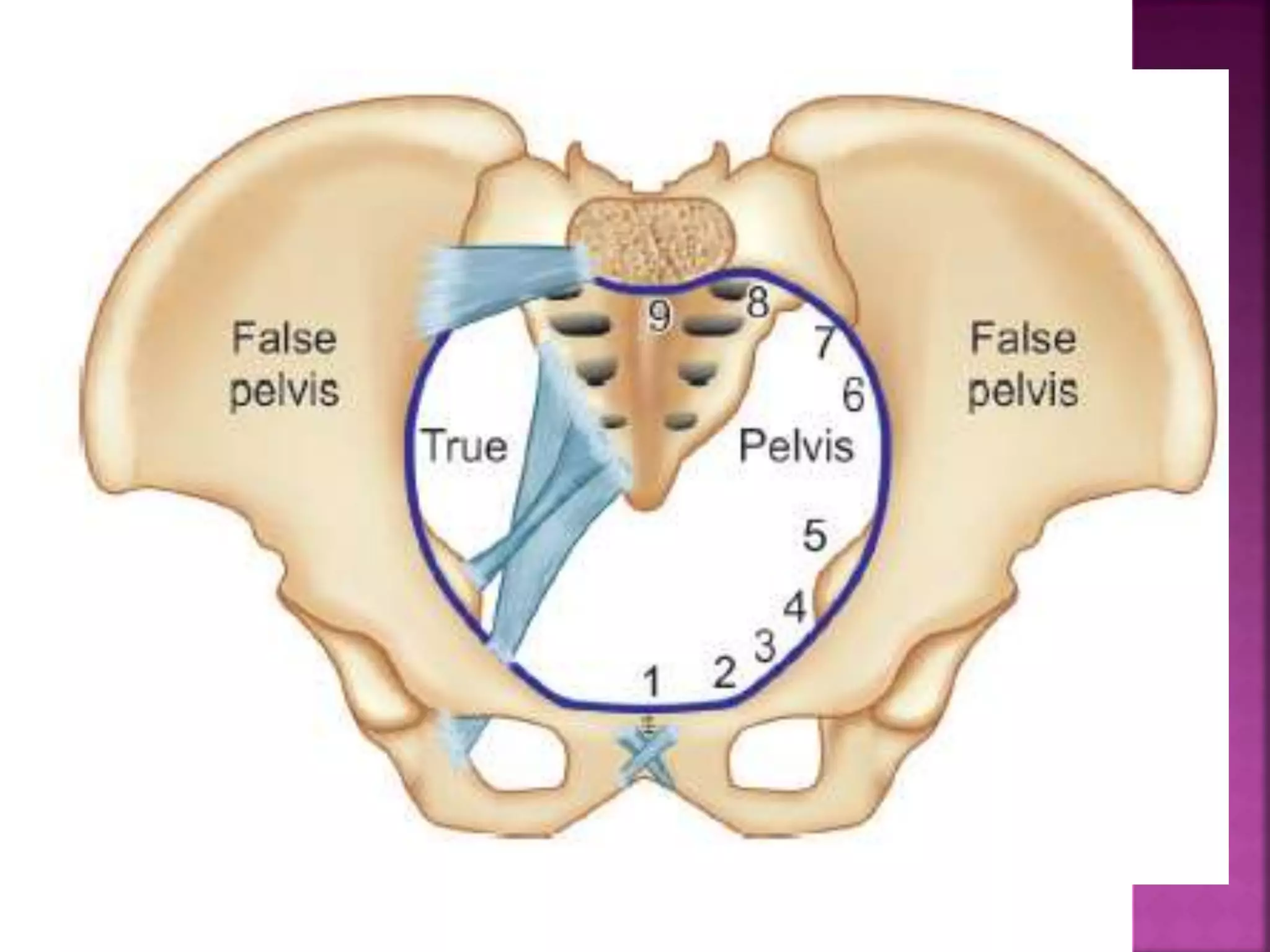


![ Inlet has 3 boundaries –
Anteriorly – symphysis pubis and horizontal
rami of pubis
Laterally – linea terminalis
Posteriorly – sacral promontory and alae of
sacrum
It has 3 diameters
1. AP dia.[3] -
2. Transverse - 13 cm – farthest pts. Of linea
3. Oblique dia- 12 cm – SI.jt to iliopectineal
eminence](https://image.slidesharecdn.com/pelvis-200323054350/75/Pelvis-Obstetrical-Significance-18-2048.jpg)
![ Antero-postero diameter has 3 diameters.
1. Obstetrical conjugate – important – from
sacral promontory to neaest point on the
post. Surface of pubis – 10 cm
2. Diagonal conjugate – clinically detected –
from sacral Promontory to lower border of SP
or apex of pubic arch – 12cm [DC-1.5 to 2cm
is obs.conj.]
3. Anatomical conjugate or conjugate vera or
true conjugate – from sacral promontory to
inner surface of upper part of sym. Pubis –
11cm](https://image.slidesharecdn.com/pelvis-200323054350/75/Pelvis-Obstetrical-Significance-19-2048.jpg)
![Transverse diameter
of inlet transects
diagonal conjugate 4
cm from sacral
promontory.[ Post.
Sagital]](https://image.slidesharecdn.com/pelvis-200323054350/75/Pelvis-Obstetrical-Significance-20-2048.jpg)









The document provides a comprehensive overview of the anatomy of the pelvis, detailing its components, including the os innominatum, sacrum, and coccyx, and describing its four main joints and various angles that influence labor mechanisms. It classifies pelvis types according to the Caldwell-Moloy classification, including gynaecoid, android, anthropoid, and platypelloid types, as well as discussing the boundaries and dimensions of the true pelvis. Additionally, the document touches upon pelvic deformities and their implications on delivery.























































































