Downloaded 285 times

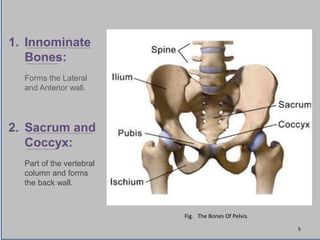

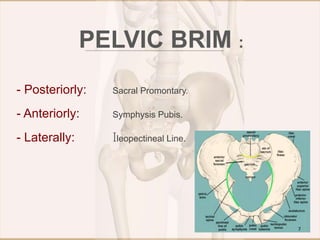
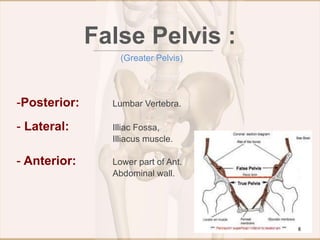
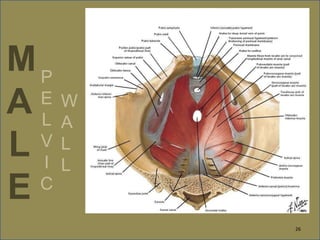
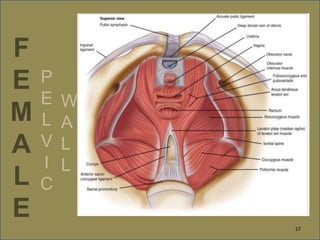
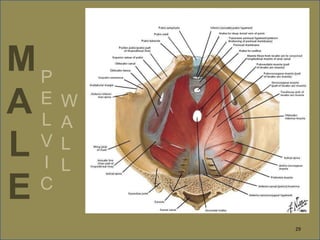
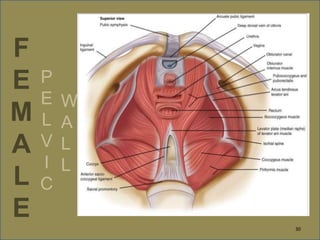
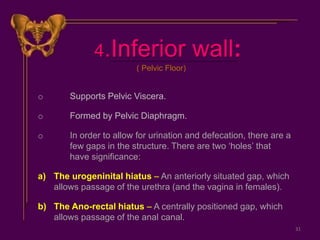
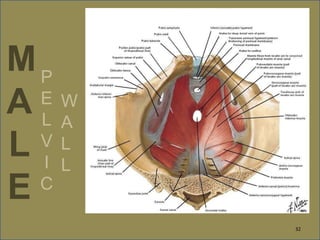
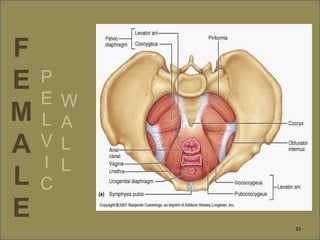
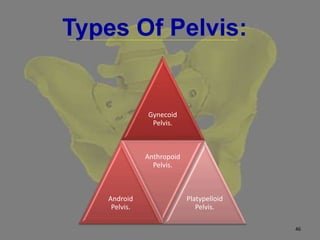

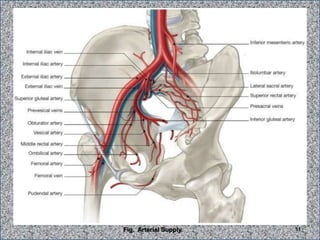
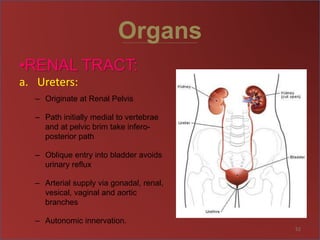
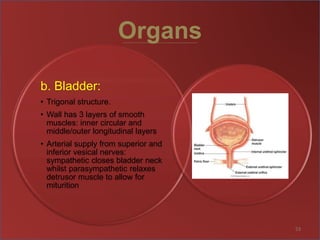
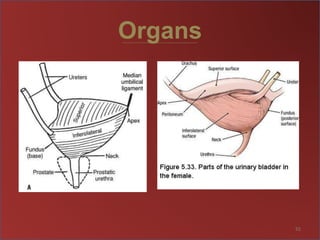
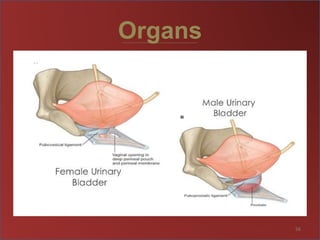
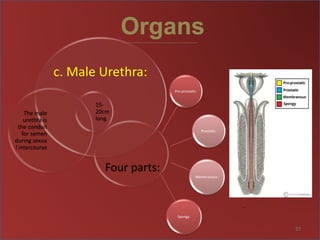
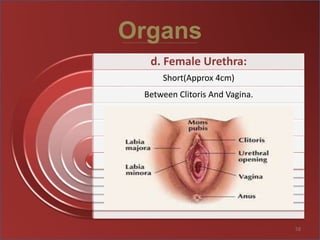
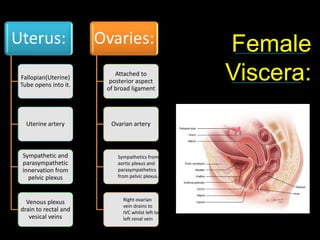
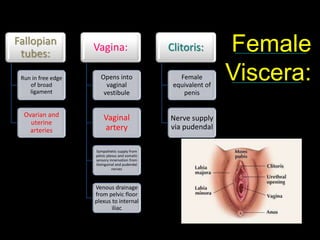


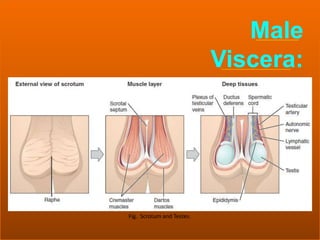
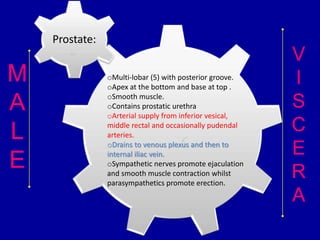
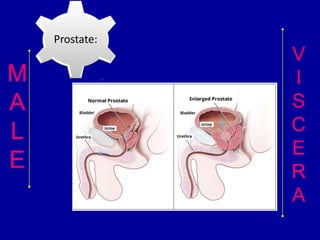
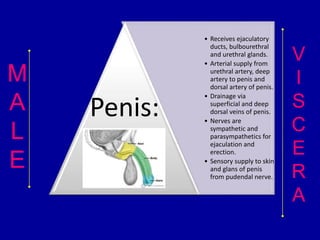
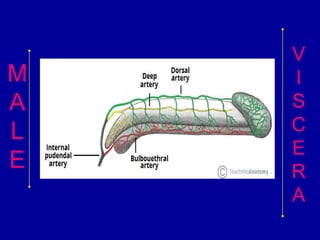


This document provides an overview of the bones and structures that make up the male and female pelvis. It discusses the bones (innominate bones, sacrum, coccyx), articulations, walls, inlet, outlet, cavity and floors of the pelvis. It also describes the muscles that comprise the pelvic diaphragm and floor. Finally, it reviews the nerves, blood vessels and organs contained within the male and female pelvis, including differences in structures like the prostate and penis in males versus the uterus, fallopian tubes and vagina in females.