Downloaded 673 times
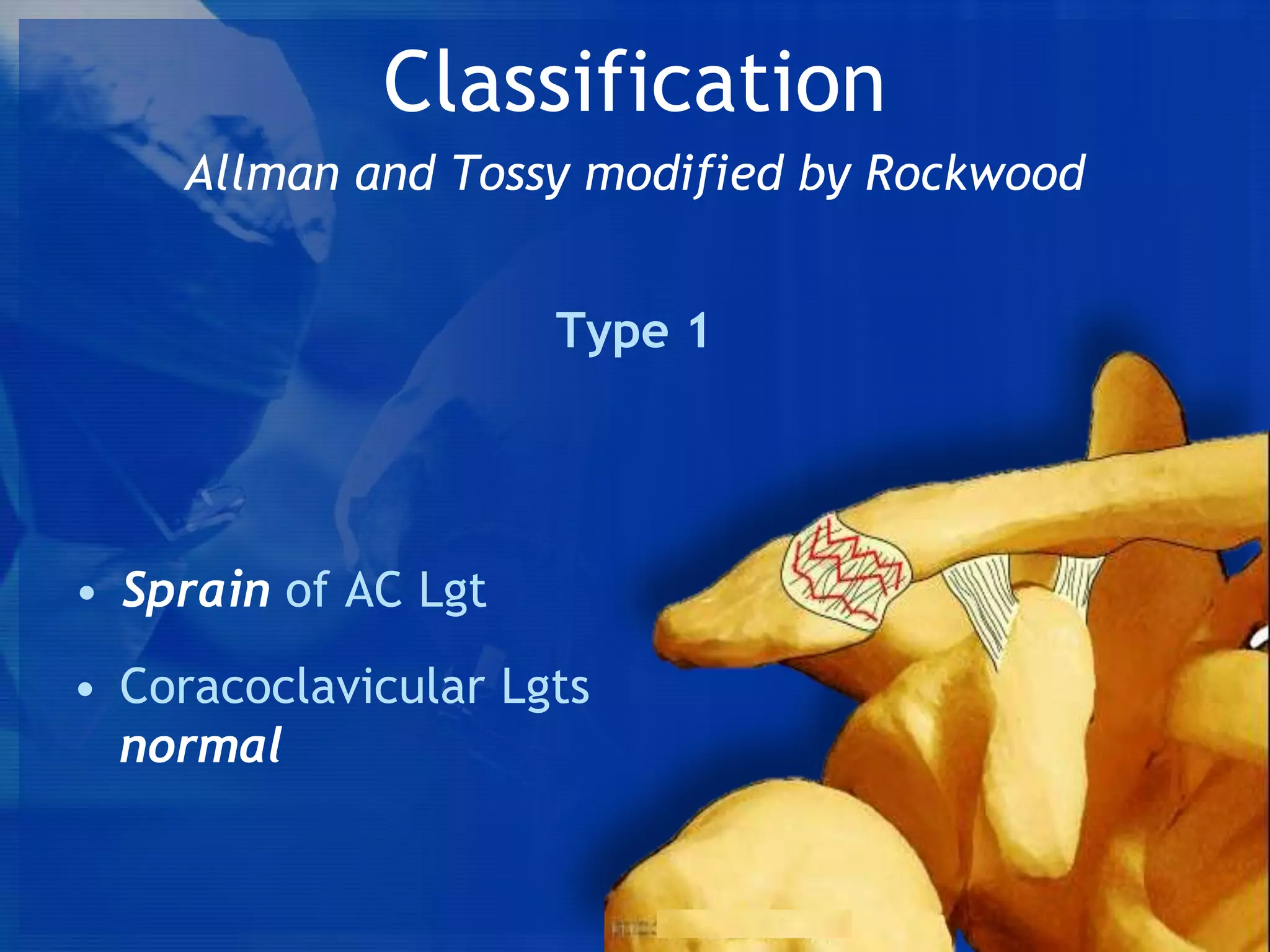
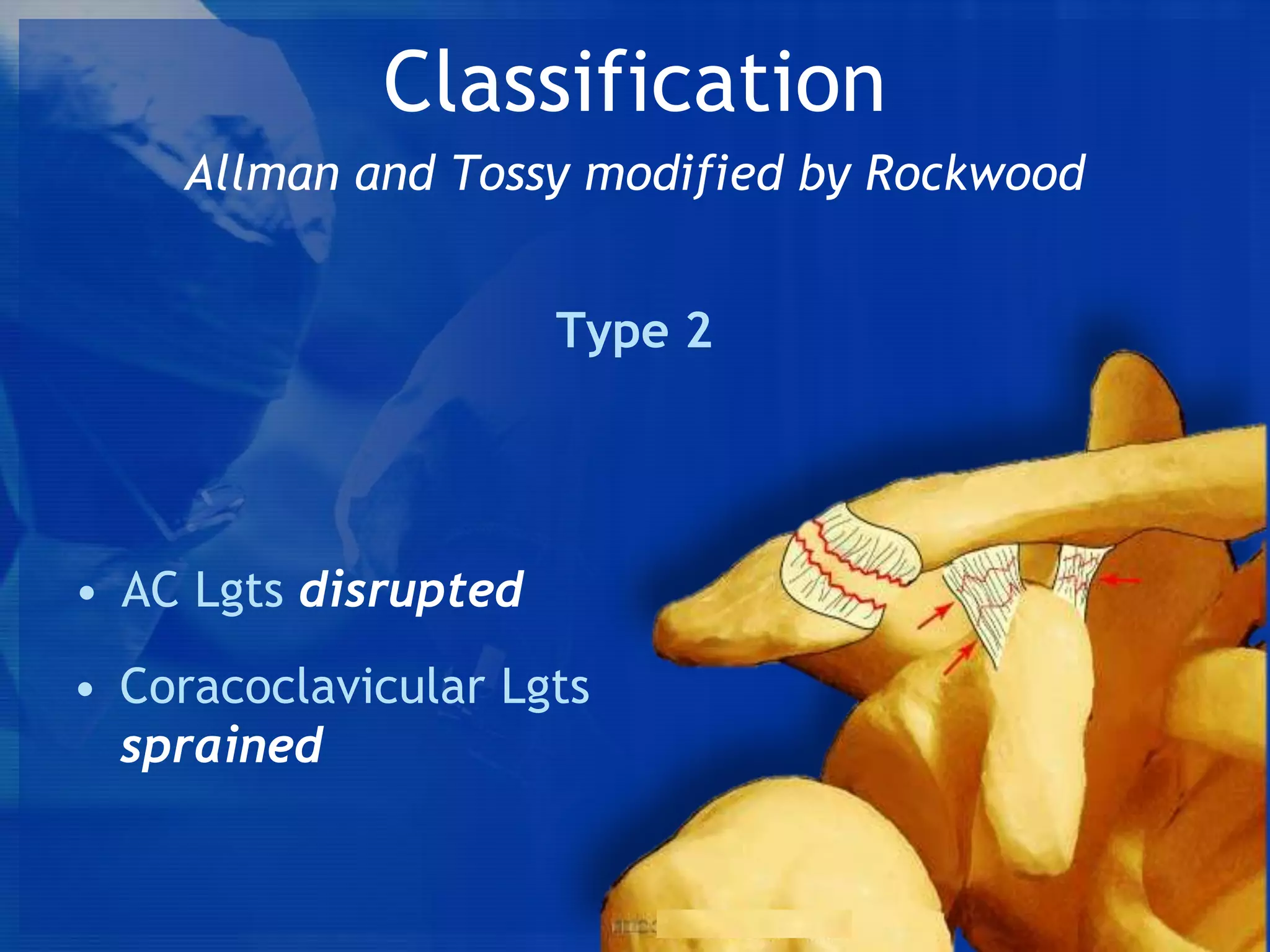

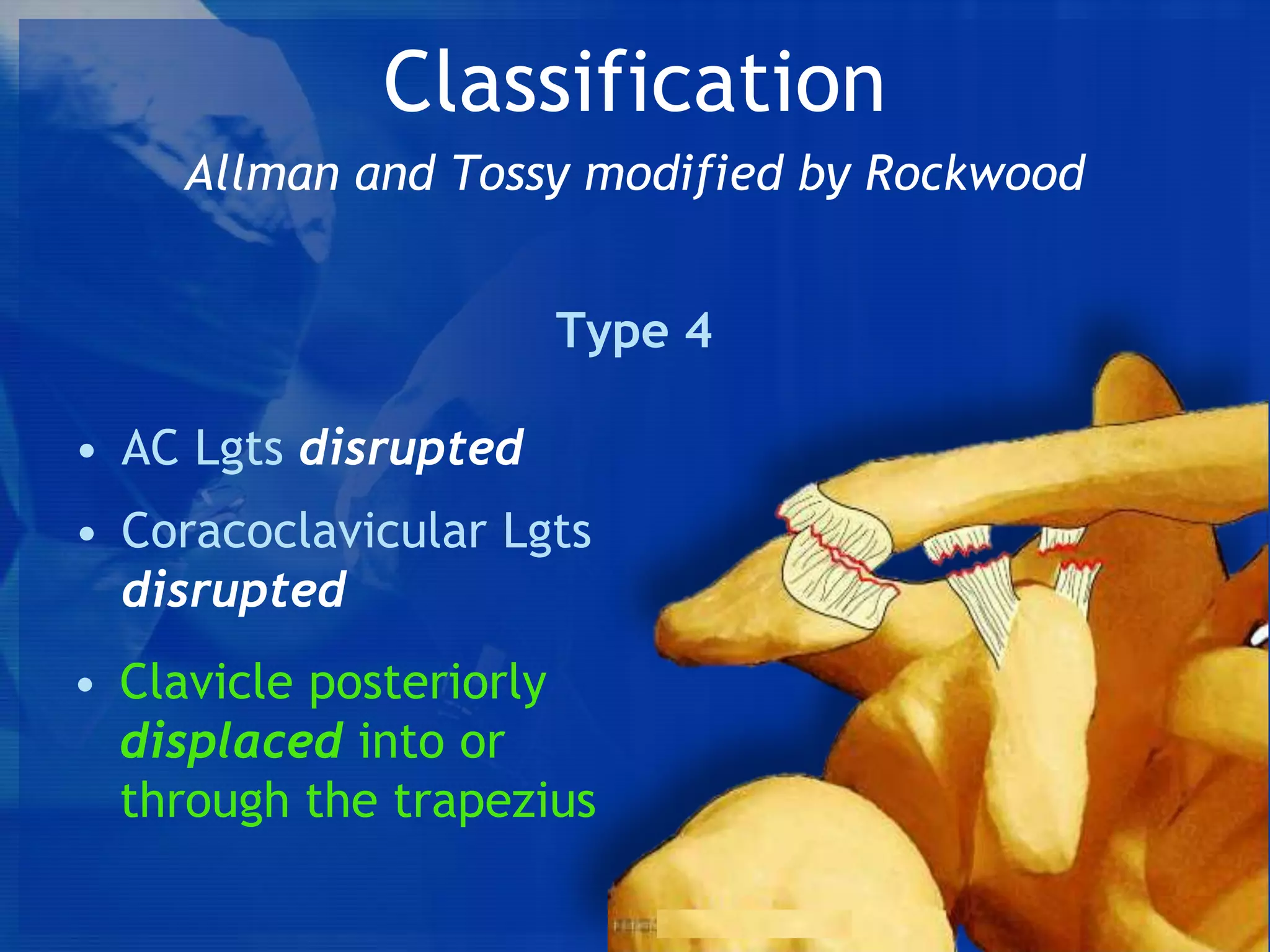
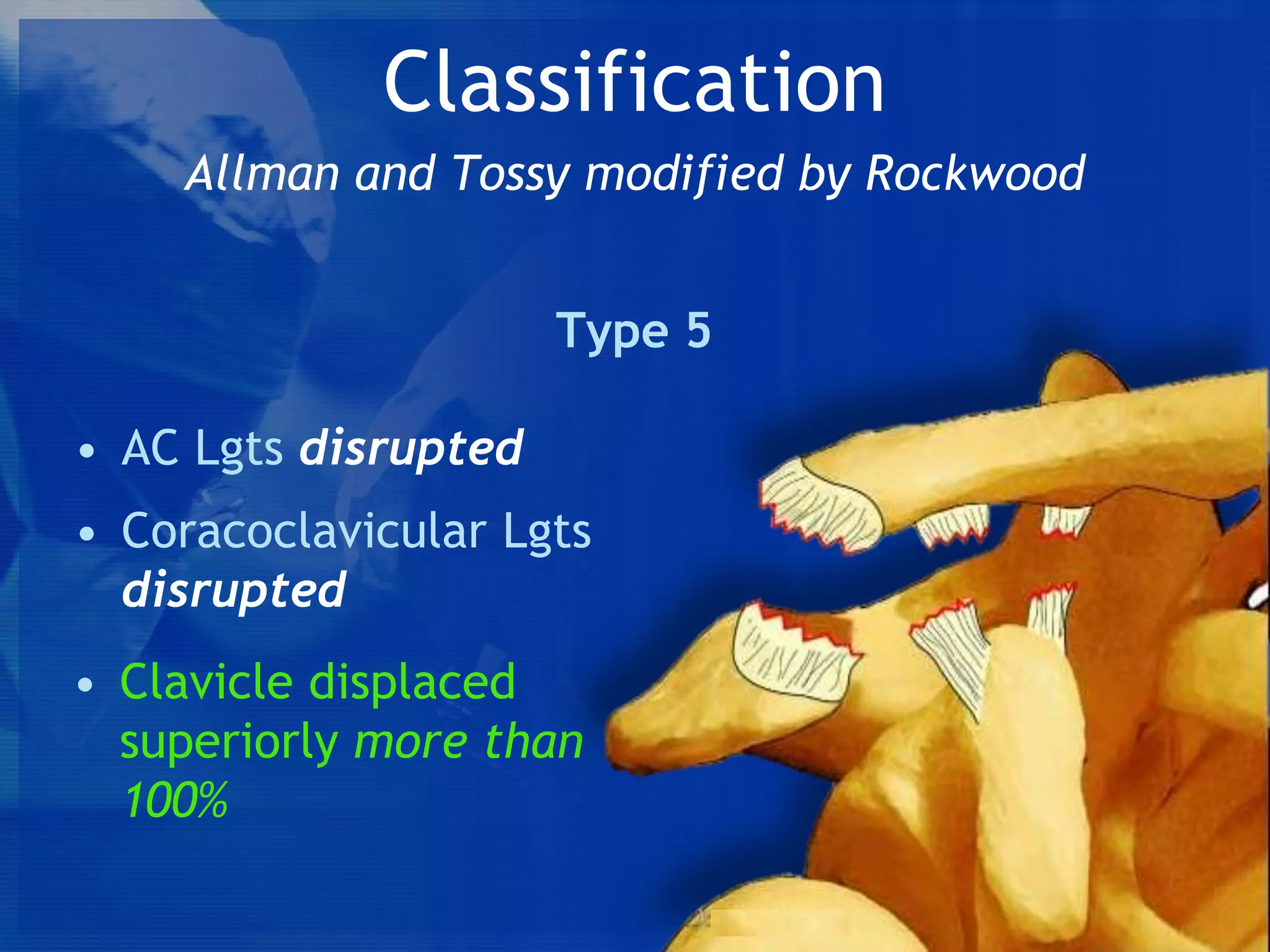
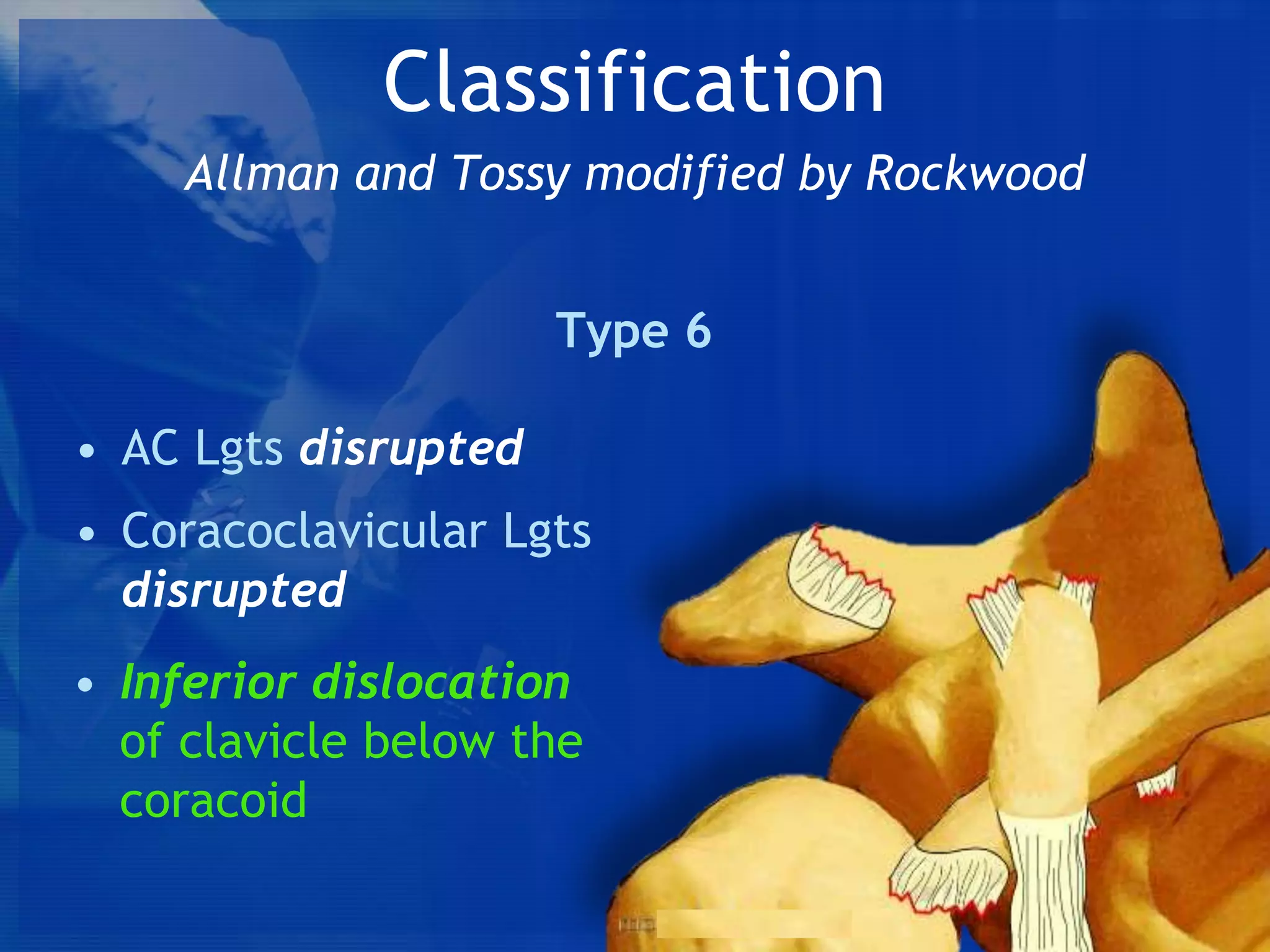
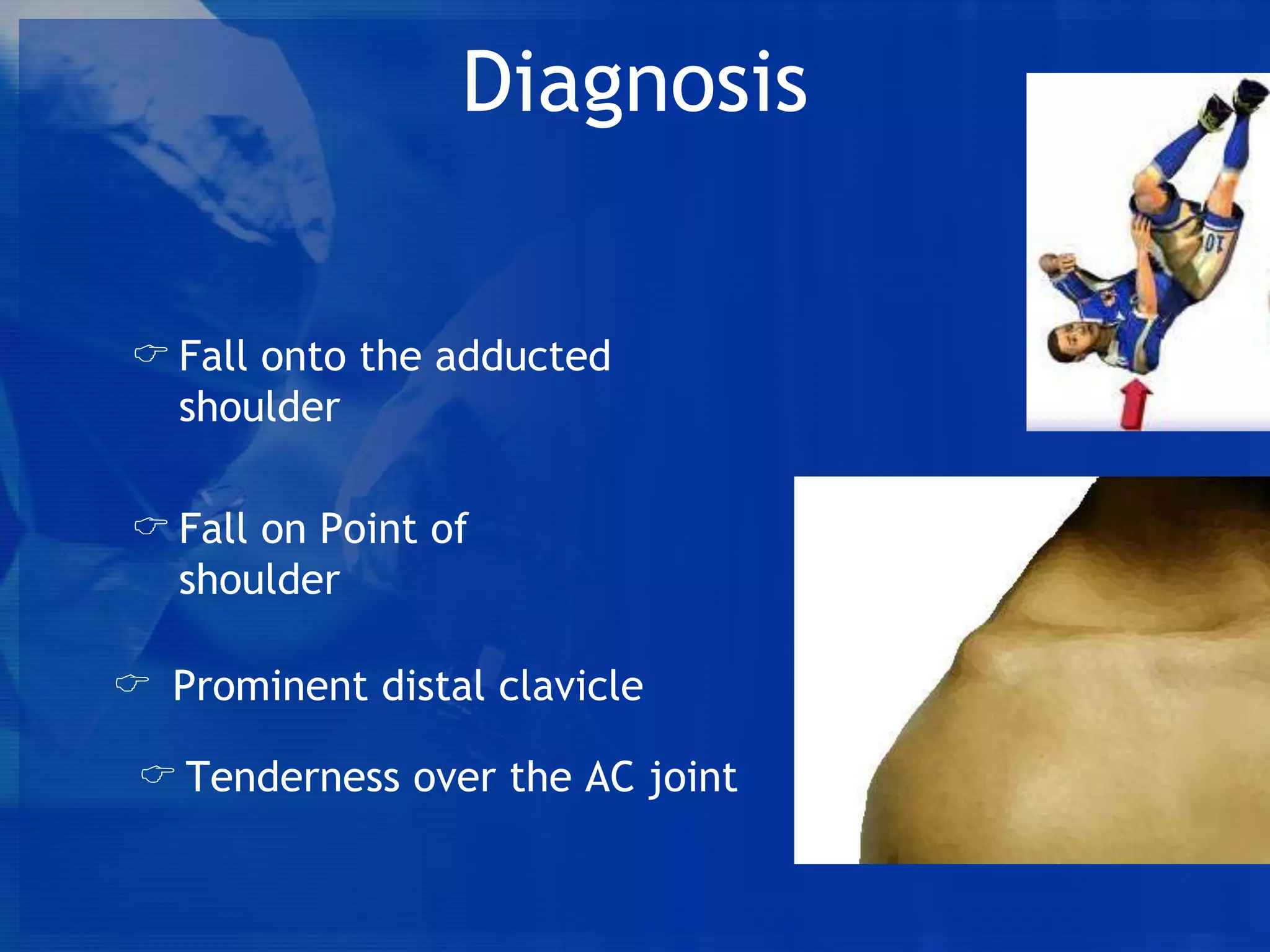


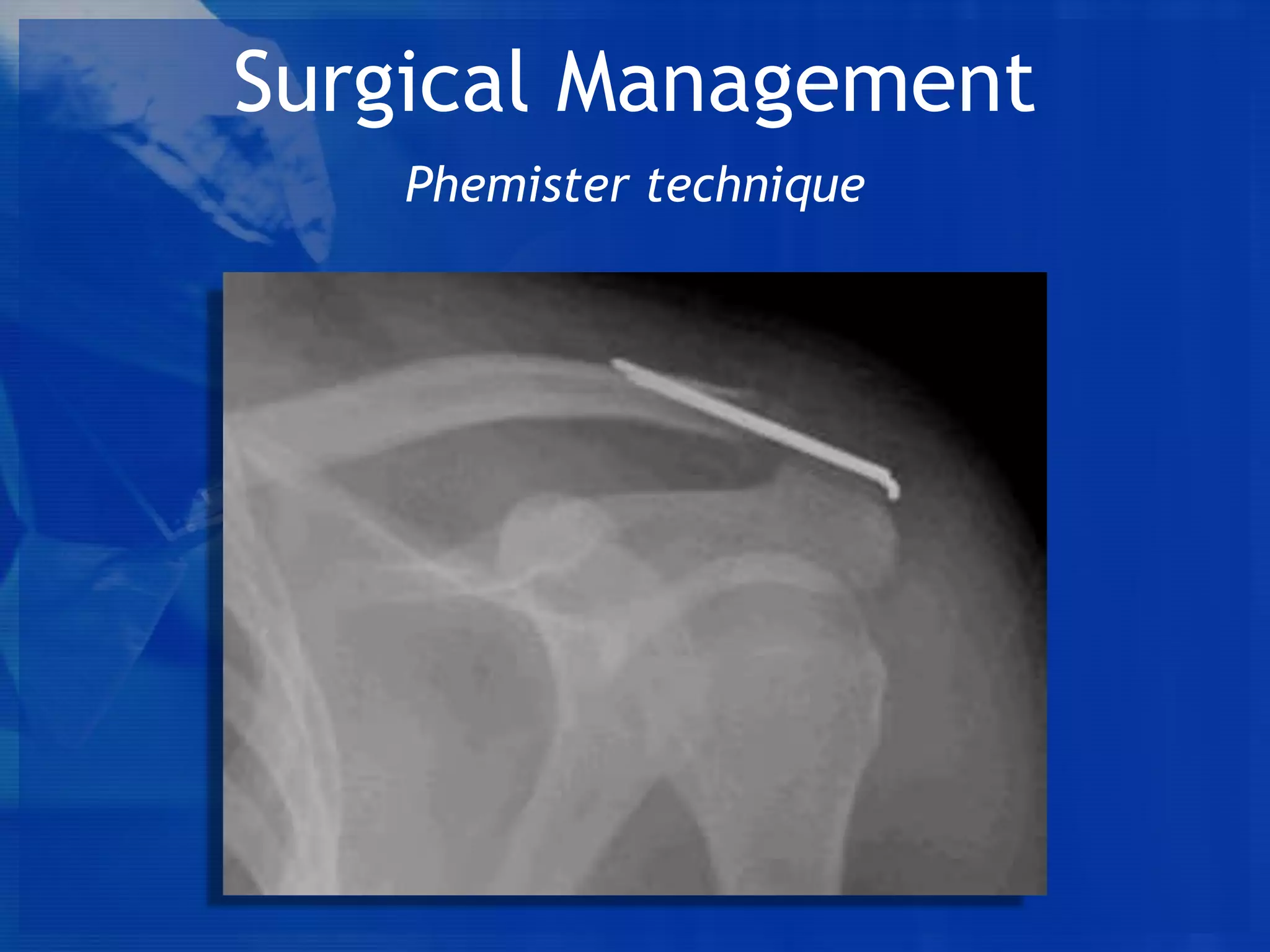
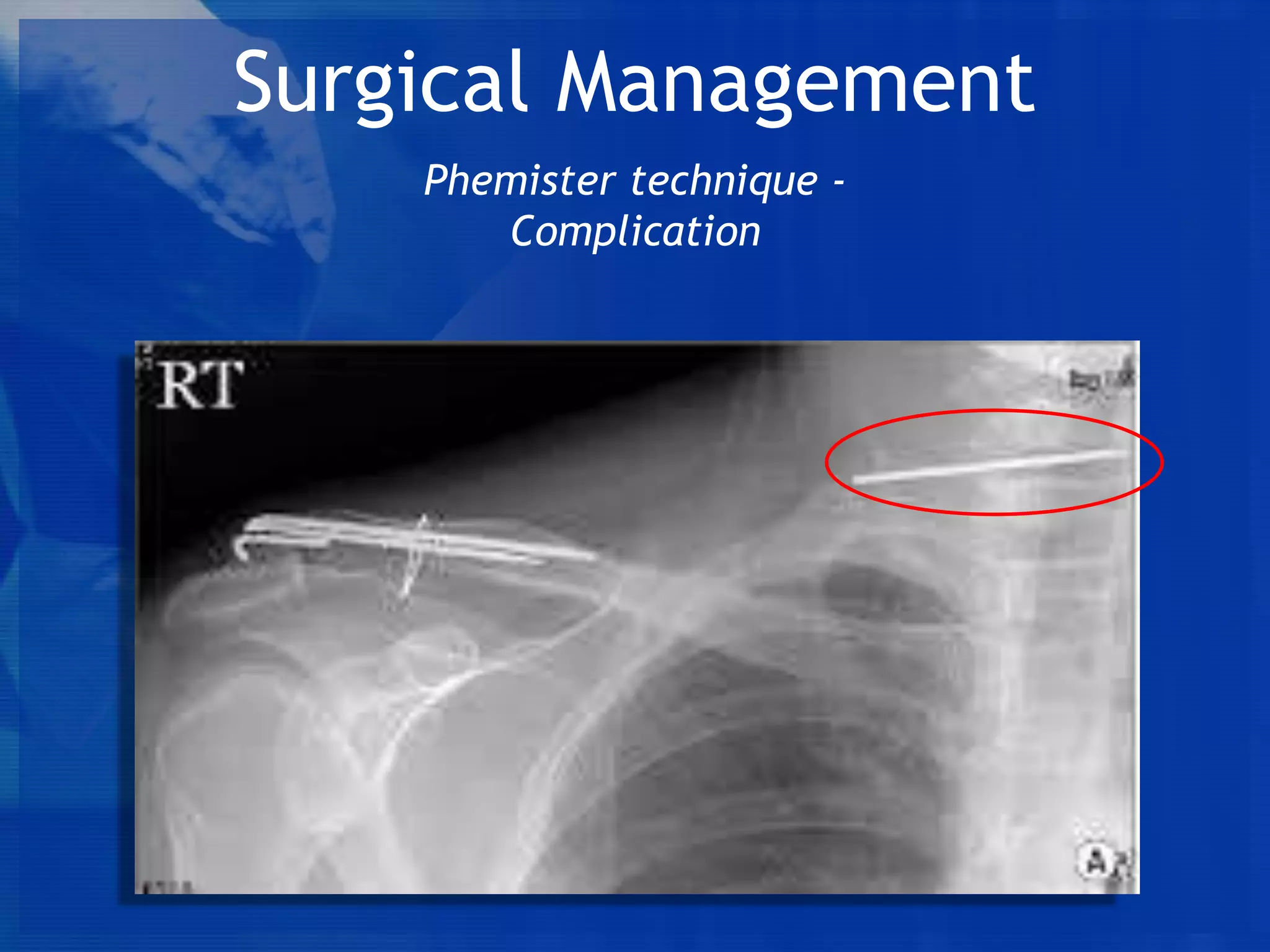
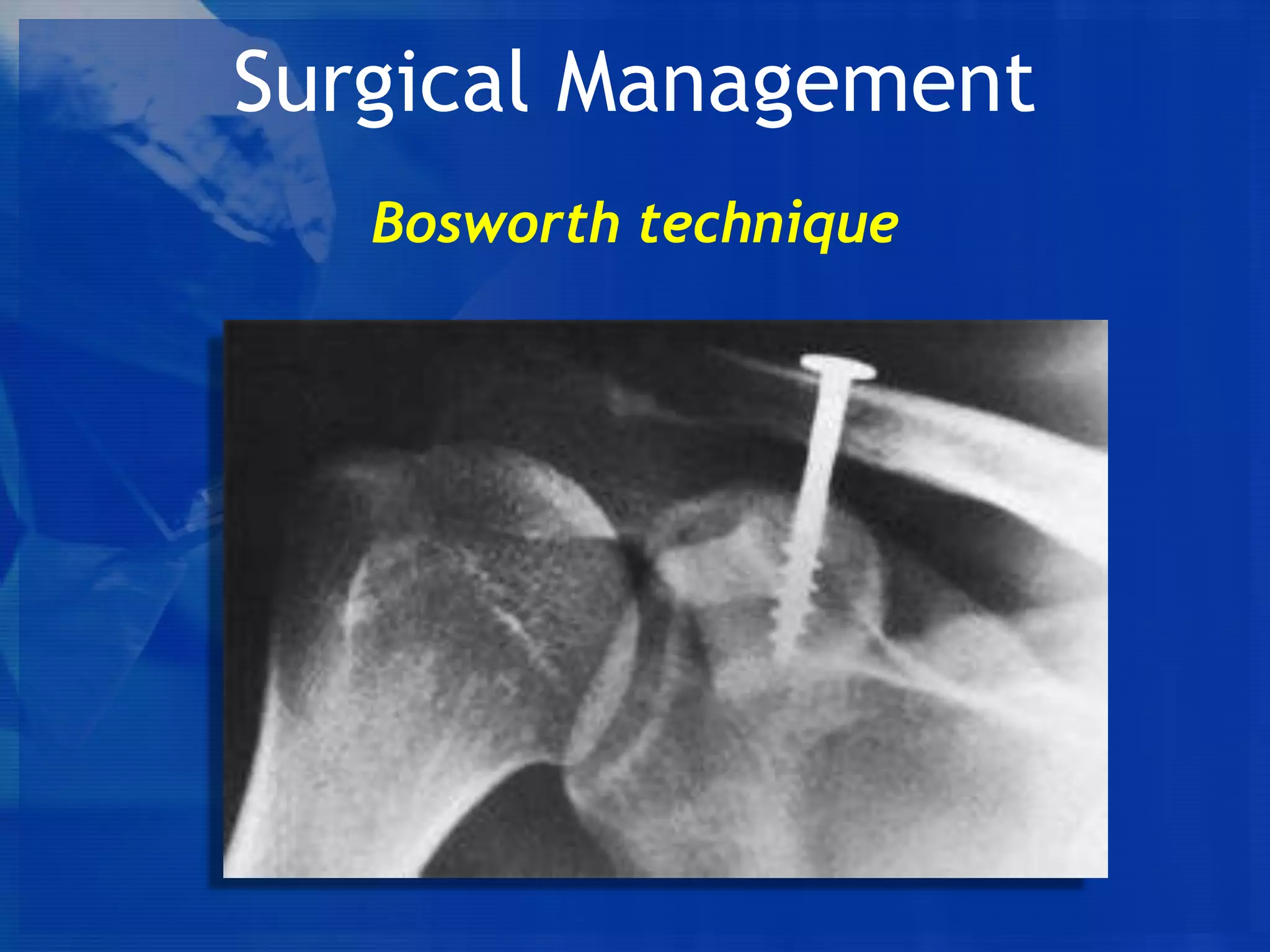
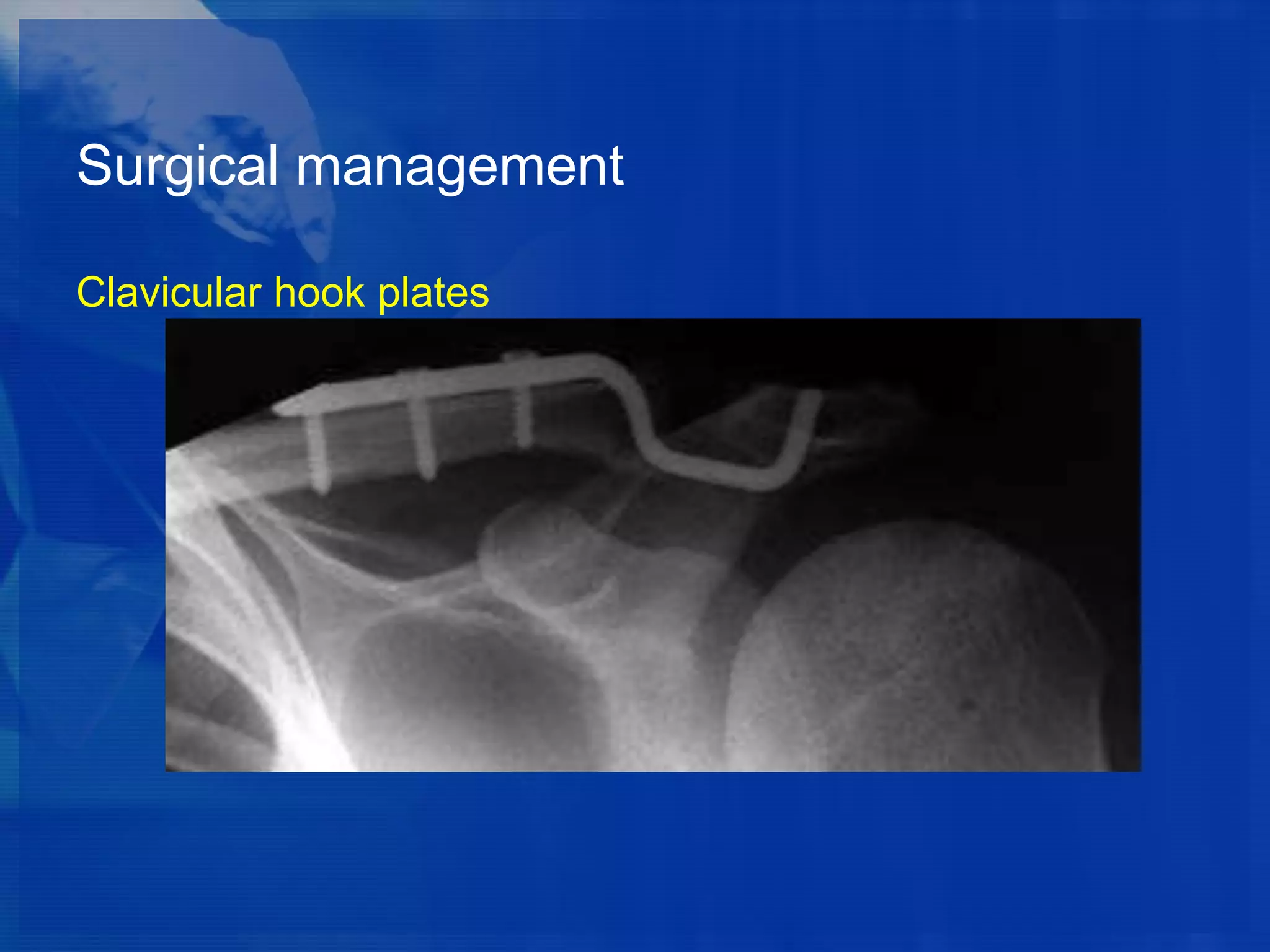


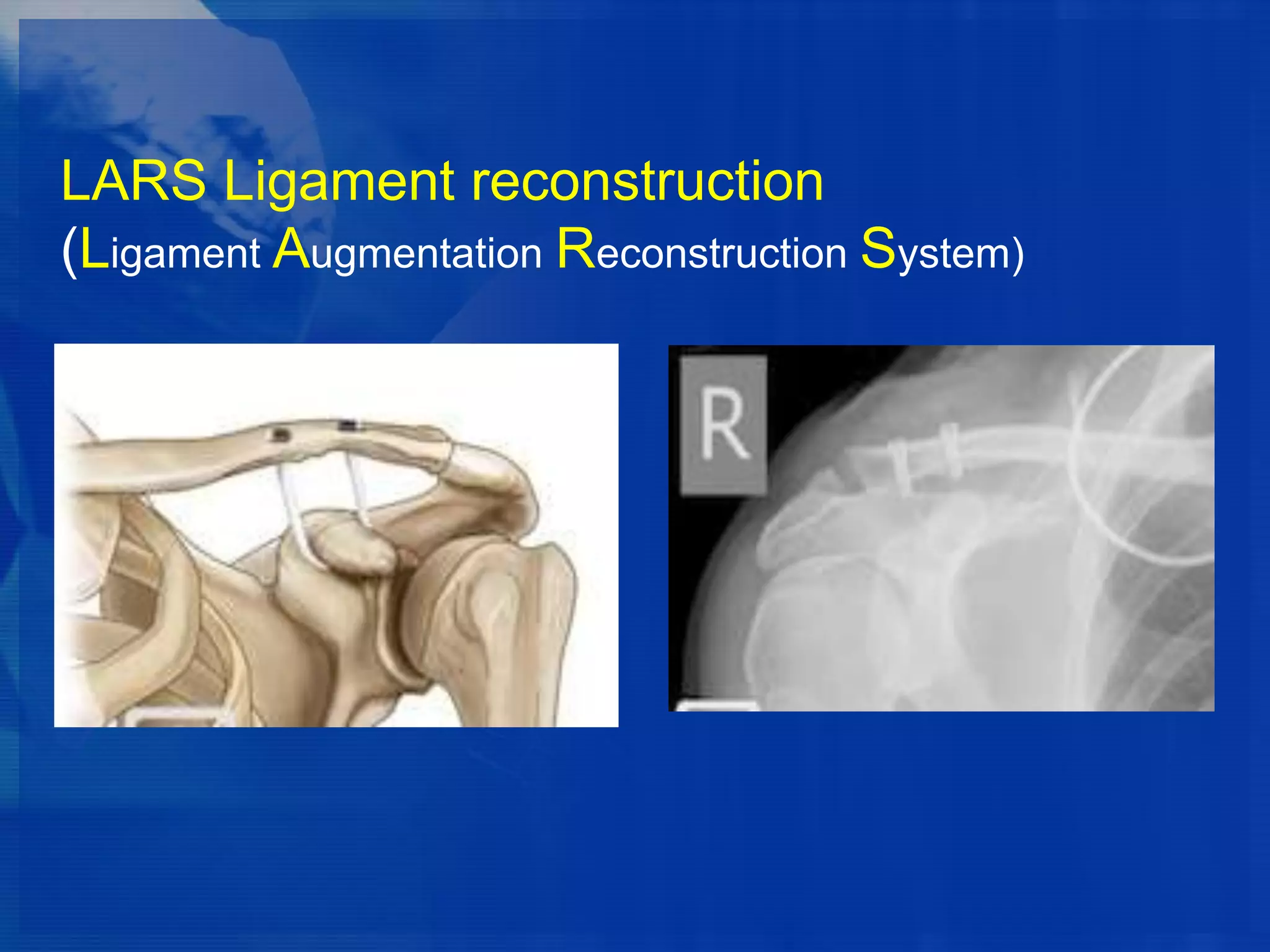







This document discusses the classification and treatment of acromioclavicular (AC) joint dislocations. It classifies AC joint injuries using the Rockwood classification system, which involves 6 types of injuries based on the degree of ligament disruption and bone displacement. For types 1 and 2 injuries, conservative treatment with rest, ice, and sling is usually recommended. Treatment for type 3 injuries is controversial but often involves initial conservative treatment with possible later surgery. Surgical treatment is described for more severe injuries. Overall, the document indicates that outcomes are often comparable between conservative and surgical treatment, but surgery carries higher risks of complications.