Downloaded 298 times
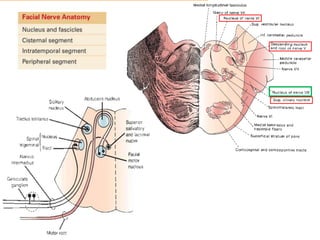
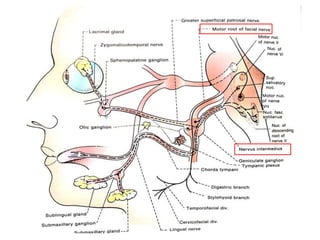
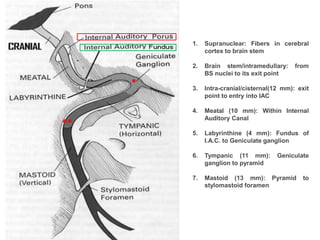
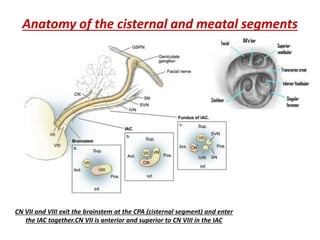
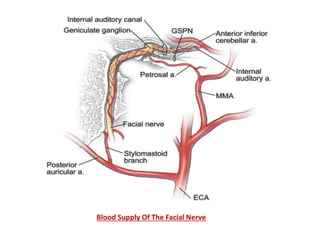
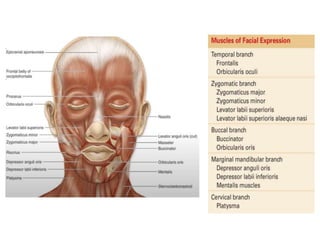
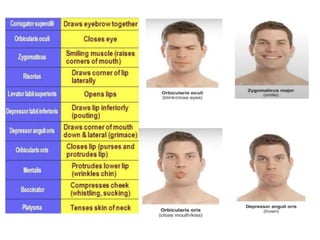
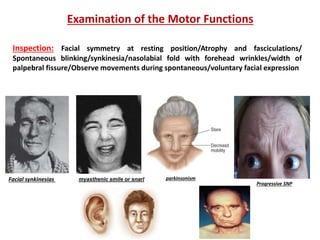
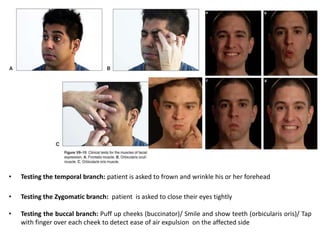
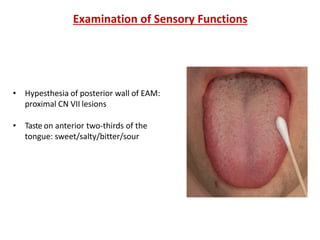
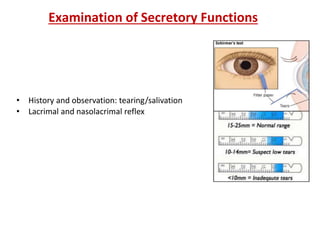
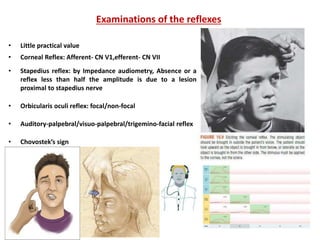
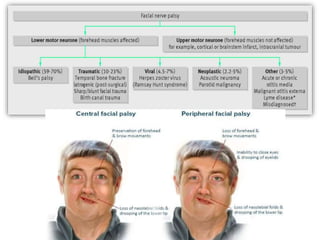
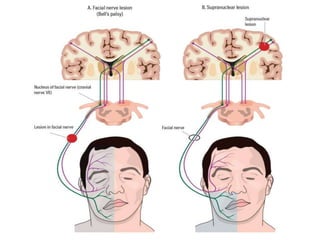
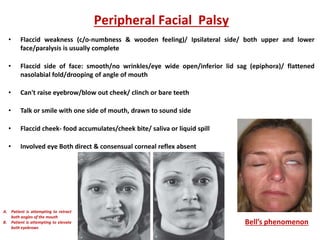
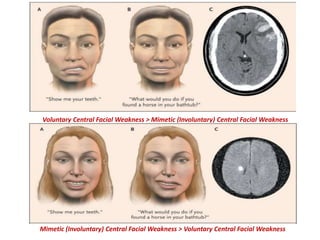
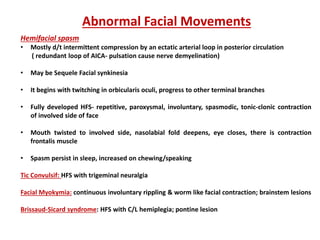
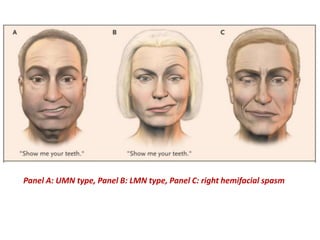
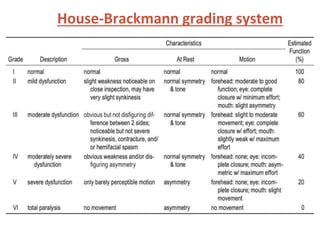
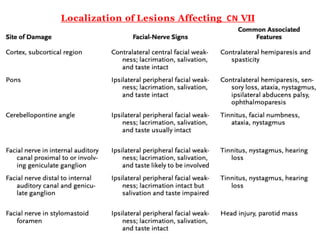

This document provides information about examining the facial nerve. It discusses the anatomy of the facial nerve and its blood supply. It then describes how to examine the motor, sensory and secretory functions of the facial nerve. Specific techniques are outlined to test different branches of the facial nerve. Disorders that can affect facial nerve function are explored such as Bell's palsy, central lesions, and abnormal facial movements. Diagrams are included to help localize lesions of the facial nerve and demonstrate types of facial weakness.