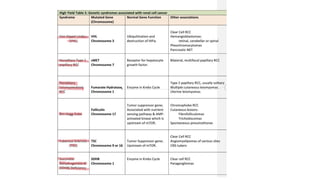
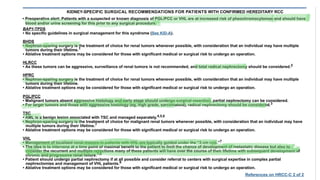
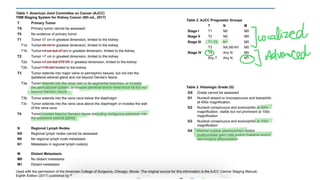
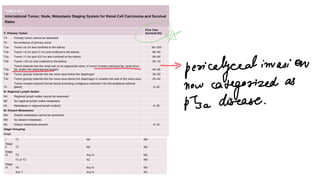
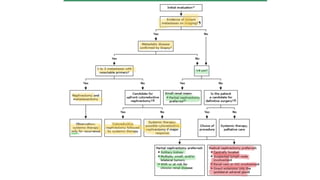
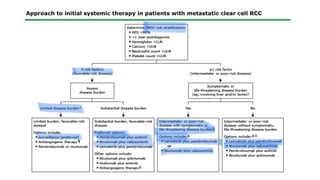
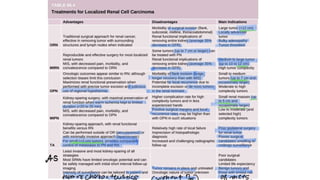
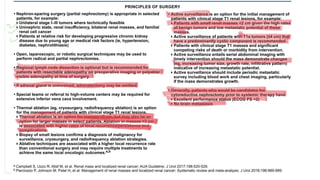
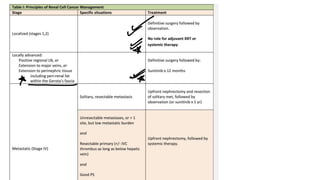
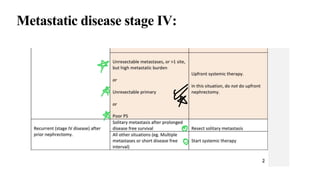
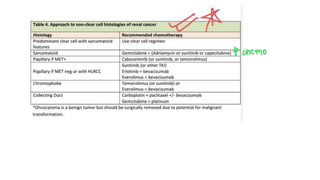
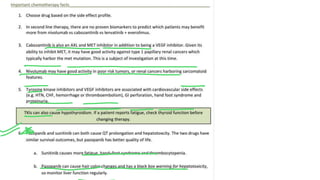
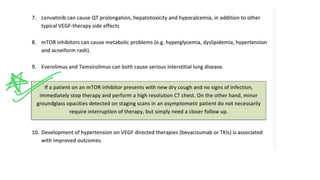
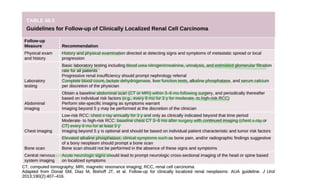
The document discusses the management of renal cell carcinomas (RCC) associated with genetic syndromes. It notes that for von Hippel-Lindau syndrome, smaller tumors less than 3 cm are observed while larger tumors greater than 3 cm are removed. For hereditary papillary RCC, surgery is emphasized to remove larger lesions and observe smaller ones due to the indolent nature of type 1 papillary RCC. For hereditary leiomyomatosis RCC, delayed intervention is not recommended due to the aggressive nature of the tumors, and wide local excision is recommended even for tumors under 3 cm. The document also discusses staging, treatment options including radical nephrectomy and minimally invasive approaches, management

















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


