Downloaded 17 times













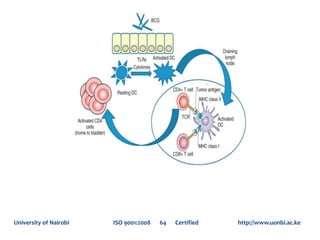







The document discusses immunotherapy in urologic oncology, including relevant immunology concepts, mechanisms of how cancer cells evade the immune system, immunotherapy strategies like therapeutic vaccination and immune checkpoint blockade, and applications of immunotherapy in renal cancer, upper tract urothelial carcinoma, bladder cancer, penile cancer, and testicular cancer. It provides details on immunotherapeutic agents and their mechanisms of action, efficacy, and side effect profiles.




































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







