This document summarizes key information about duodenal injuries:
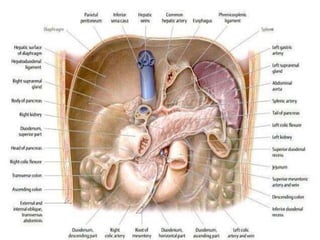
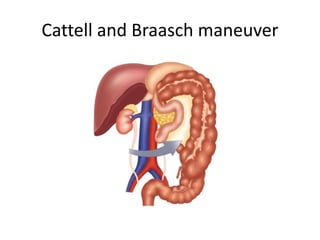
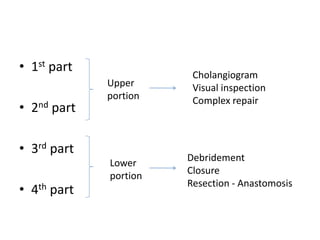
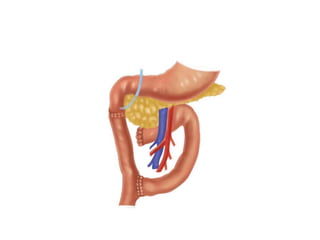
- The duodenum is 12 inches long and located retroperitoneally behind the liver and pancreas. It has four parts and is vulnerable to trauma due to its location and proximity to other abdominal organs.
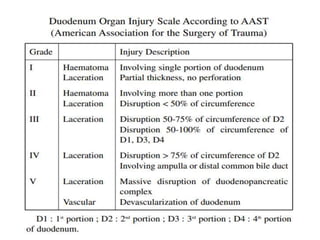
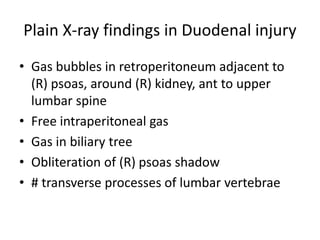
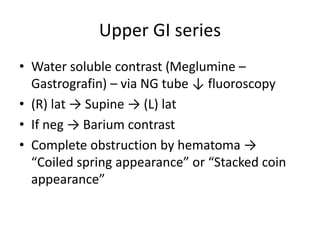
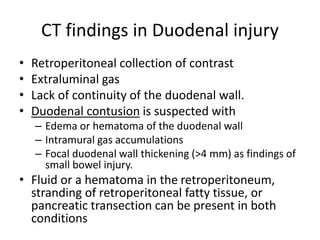
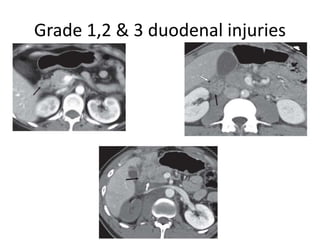
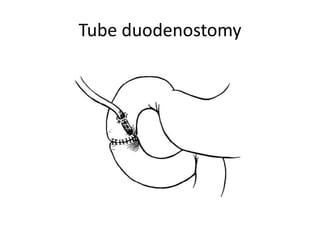
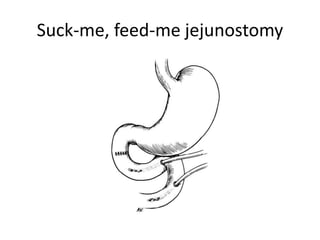
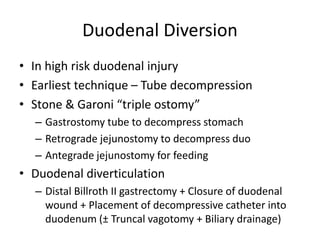
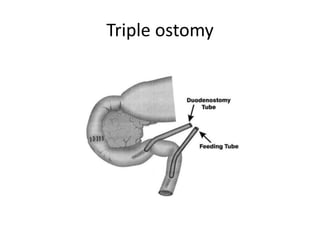
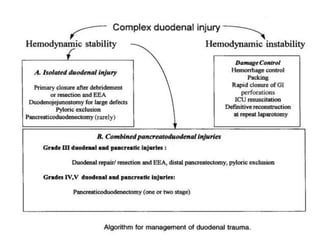
- Duodenal injuries can be from penetrating or blunt trauma. Diagnosis involves imaging like CT scans and upper GI series. Management principles involve restoring intestinal continuity, decompressing the duodenum, providing drainage, and nutritional support.
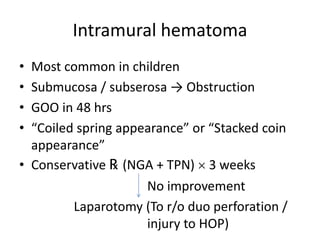
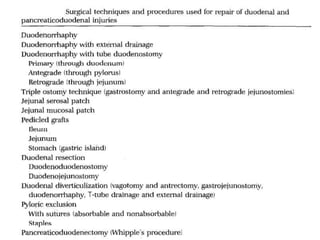
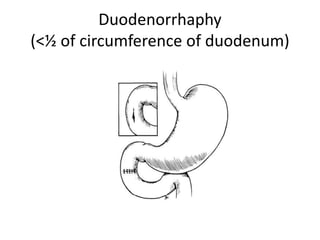
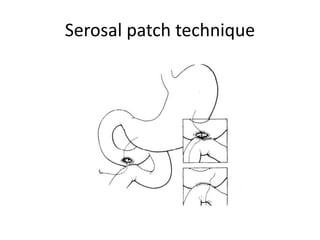
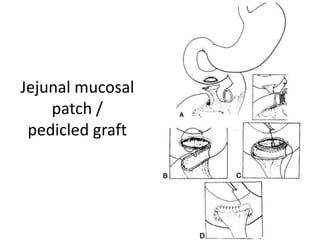
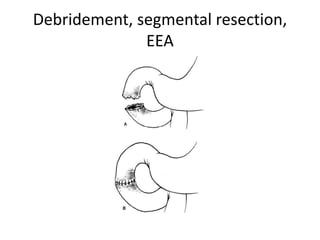
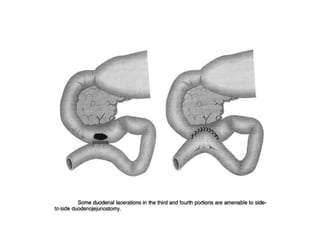
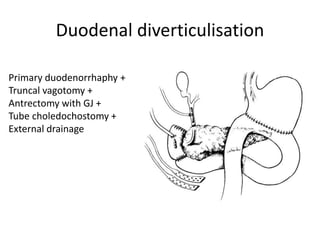
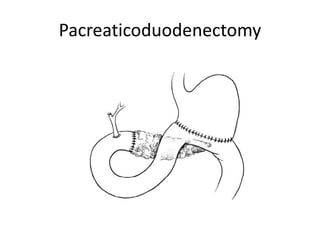
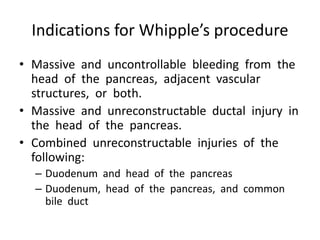
- Treatment options depend on the severity of injury and include primary repair, diversion procedures like gastrojejunostomy, or pancreaticoduodenectomy for severe injuries involving other structures. Complications can include