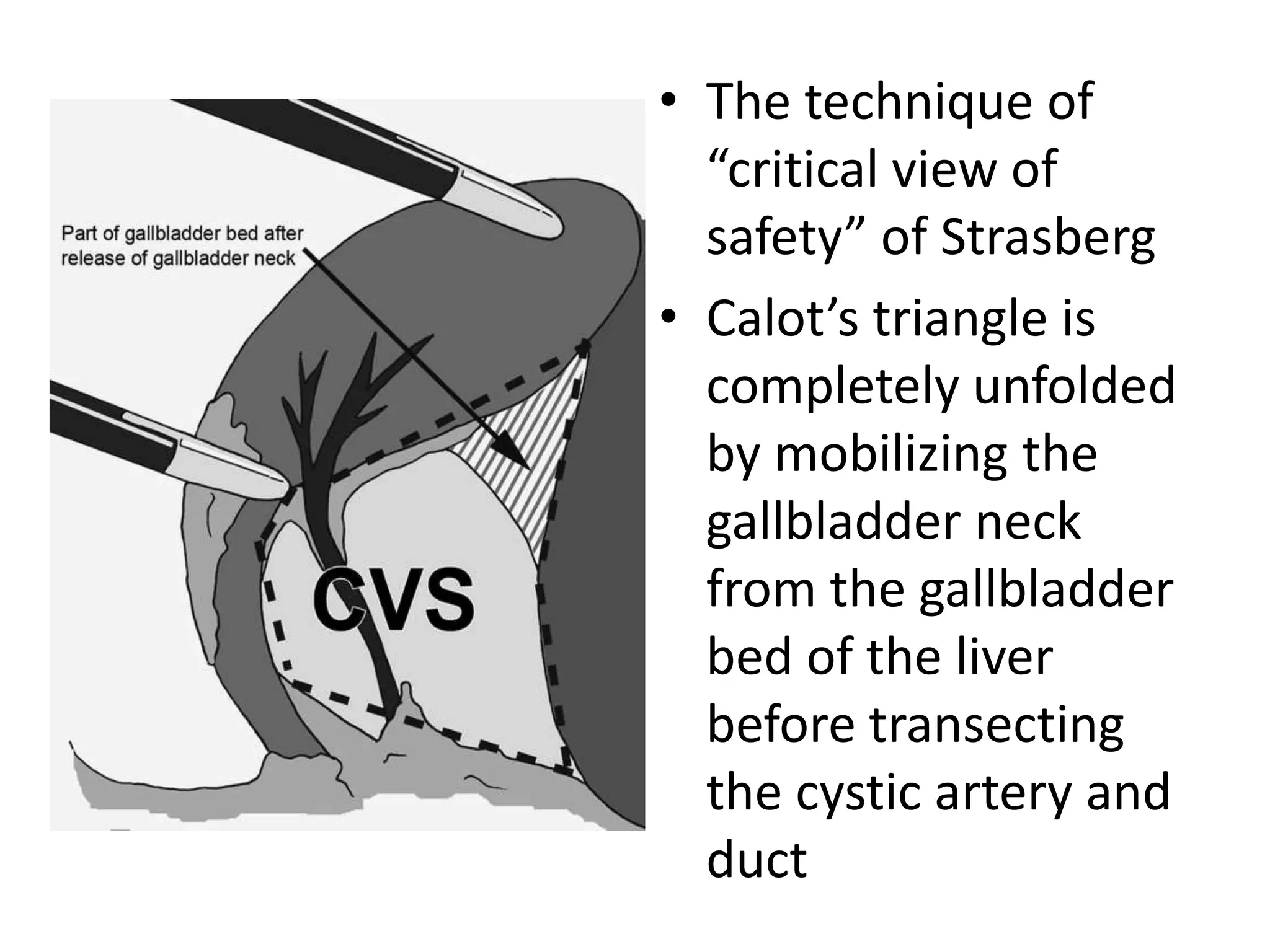
Bile duct injuries are a complex complication seen more frequently with laparoscopic cholecystectomies due to aberrant anatomy and increased procedures. They can involve the cystic duct, gallbladder bed, or major bile ducts. Various classification systems exist to describe the level and extent of injury. Injuries may be detected intraoperatively by cholangiogram abnormalities, bile drainage from unusual locations, or anomalous anatomy. Prevention strategies include proper case selection, opening retroperitoneal folds, dissecting close to the gallbladder, achieving the critical view of safety, and using intraoperative cholangiography.