This document discusses the pharmacology of sedatives and hypnotics, detailing their definitions, classifications, pharmacological actions, and adverse effects. It highlights the differences between sedatives and hypnotics, the mechanisms of action for various drug classes (including benzodiazepines and barbiturates), and their uses in clinical practice. Additionally, it covers pharmacokinetics, interactions, and the role of melatonin in sleep regulation.
![► Sleep
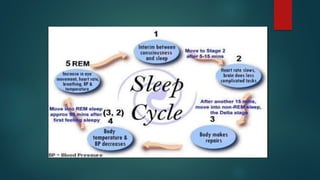
1. NREM – In this there is no fast movement of eyes.It occurres between stage 0 to 4
2. REM – In this eye movements are very fast.
► Stage of NREM-
► Stage 0 [ awake]- It is condition from lying down to falling a sleep(1-2%)
► Stage 1 [dosing]– Eye movement decrease,body muscles relax (5-10%)
► Stage 2 [unequivocal sleep]– more decrease in eye movements, person may arousable.(50%)
► Stage 3 deep sleep transition]– Deeper sleep with minimum eye movements,not easily arousal.
► Stage 4[cerebral sleep] – deepest level of sleep, GH secretion increased, no eye movements, muscles are
fully relaxed, if awakened causes disorientation.(20%)
► REM – dreaming, HR,breathing rate, brain activity increases and relaxation of voluntary muscles.](https://image.slidesharecdn.com/hypnoticsbyapurva-220326060300/85/hypnotics-by-apurva-pdf-6-320.jpg)