2
PFT:
• Indicate aset of manoeuvres that are performed
by the patient or by using standardized equipment
to measure lung function
• Evaluates one or more aspects of respiratory
system
• Respiratory mechanics
• Lung parenchymal function/gas exchange
• Cardiopulmonary interaction
3.
Indications for PFT
DiagnosticPrognostic
Evaluation of signs and symptoms Assess severity
Screening at risk patients Follow response to therapy
Measure the effect of disease on
pulmonary function
Determine further treatment
goals
Assess preoperative risk Evaluating degree of
disability
Monitor pulmonary drug toxicity
4.
Indications for PFT( American college of Physicians guidelines)
• Lung resection
• H/O smoking ,dyspnoea
• Cardiac surgery
• Upper abdominal surgery
• Lower abdominal surgery
• Uncharacterized pulmonary disease(defined as history of pulmonary disease or
symptoms and no PFT in last 60 days)
5.
Contraindications
• Recent eyesurgery
• Thoracic, abdominal and cerebral aneurysms
• Active hemoptysis
• Pneumothorax
• Unstable angina/recent MI within a month
• Pregnancy( relative)
7
Categorization of
PFT’s
• GasExchange tests
• Alveolar-arterial PO2 gradient
• Diffusion Capacity
• Gas distribution tests:
1. Single breath N2
2. Multiple breath N2 test
3. Helium dilution
4. Radio Xe Scintigram
8.
• Cardio-pulmonary interaction
•Qualitative tests:
1. History and examination
2. ABG
• Quantitative tests:
1. 6 min walk test
2. Stair climbing test
3. Shuttle walk
4. CPET (cardiopulmonary exercise testing)
9.
Bedside PFTs
• RespiratoryRate
• Single breath count
• Sabrasez breath holding test
• Schneider’s Match Blowing test
• Cough test
• Forced expiratory time
• Wheeze test
• Maximum Laryngeal height
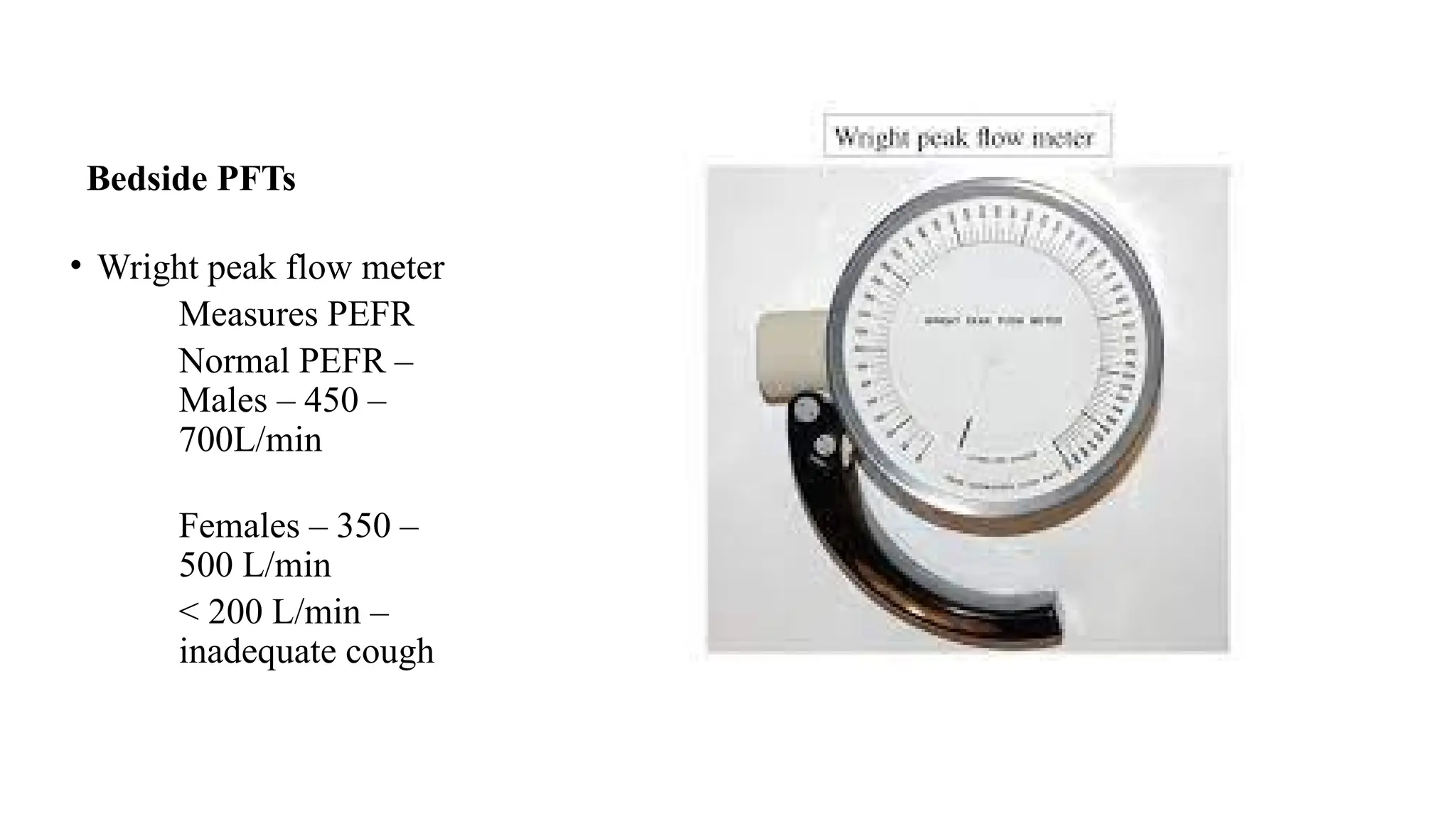
• Wright peak flow meter
• De-bono whistle blowing test
• Bedside Pulse oximetry
10.
Bedside PFTs
• RespiratoryRate:
1. Essential yet frequently undervalued
component of PFT
2. Important evaluator in weaning &
extubation protocols
3. Increase RR- muscle fatigue- work
load- weaning fails
11.
Bedside PFTs
• Singlebreath count
1. After deep breath, hold it and start
counting till next breath
2. Normal- 30-40 counts
3. Indicates Vital capacity
4. Less than 15 indicates severe
impairment of VC
12.
• Sabrasez breathholding test
1. Ask the patient to take a full but not too deep breath & hold it as long as
possible
2. >25 sec- Normal cardiopulmonary reserve (CPR)
3. 15-25 sec- limited CPR
4. <15 sec- very poor CPR ( contraindication for elective surgery)
25-30 sec- 3500ml VC
20-25 sec – 3000ml VC
15-20 sec- 2500ml VC
10-15 sec – 2000ml VC
5-10 sec – 1500ml VC
13.
Bedside PFTs
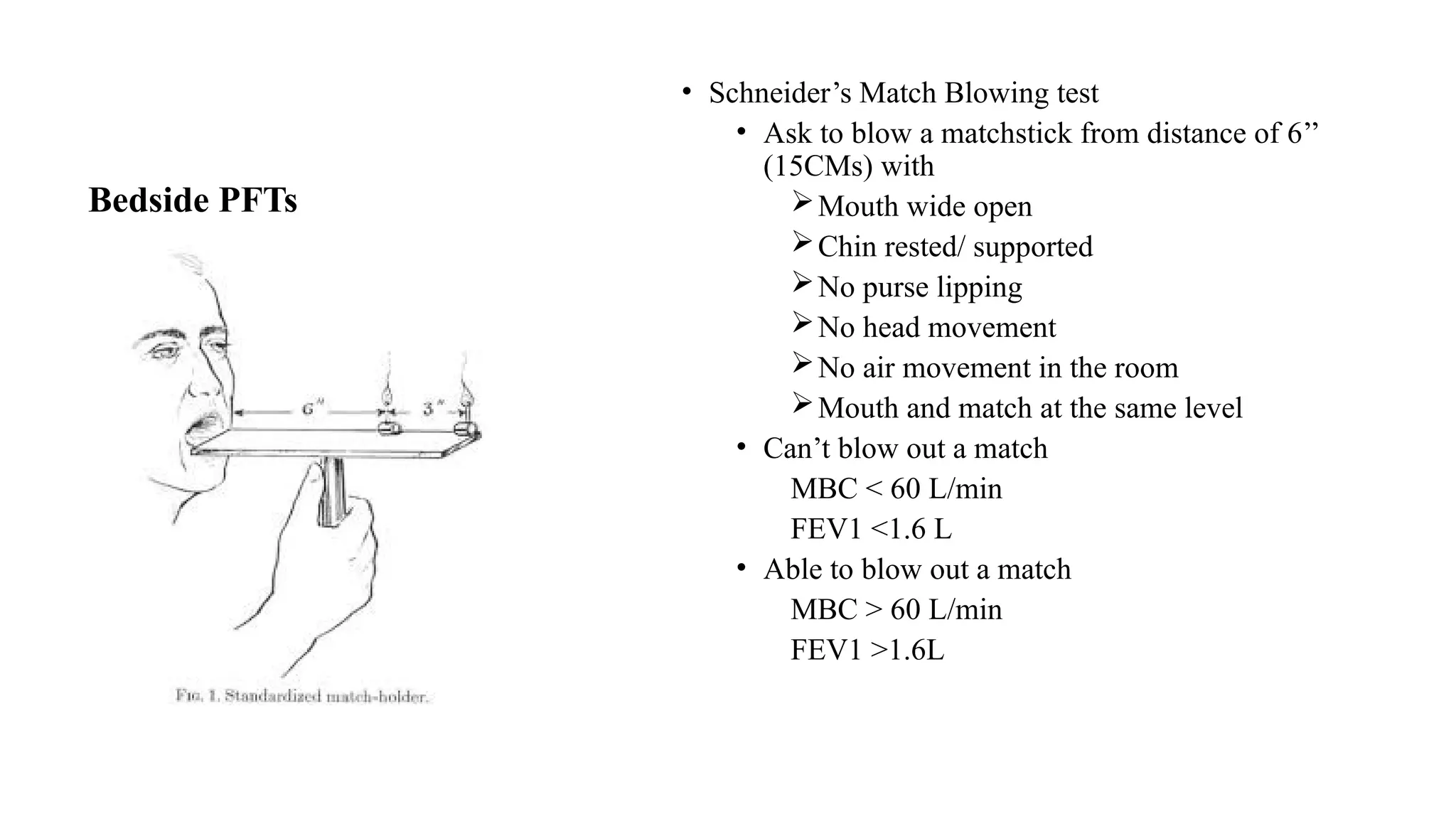
• Schneider’sMatch Blowing test
• Ask to blow a matchstick from distance of 6’’
(15CMs) with
Mouth wide open
Chin rested/ supported
No purse lipping
No head movement
No air movement in the room
Mouth and match at the same level
• Can’t blow out a match
MBC < 60 L/min
FEV1 <1.6 L
• Able to blow out a match
MBC > 60 L/min
FEV1 >1.6L
14.
Bedside PFTs
• Coughtest: Deep breath f/b cough
Ability to cough
Strength
Effectiveness
Inadequate cough if
FVC <20ml/kg
FEV1 <15ml/kg
PEFR < 200L/min
15.
23/02/2025
Bedside PFTs
• Forcedexpiratory time:
• After deep breath, exhale maximally and
forcefully
• Keep stethoscope over trachea & listen
Normal FET – 3 – 5 sec
Obstructive Lung diseases: >6 sec
Restrictive lung diseases: < 3 sec
16.
23/02/2025
Bedside PFTs
• Wheezetest:
• Five deep inspirations & expirations,
auscultate between the shoulder blades
posteriorly- presence of wheeze- indicates
positive test
• Maximum Laryngeal height:
• Distance between the upper border of thyroid
cartilage and suprasternal notch- < 4cms is
abnormal
Bedside PFTs
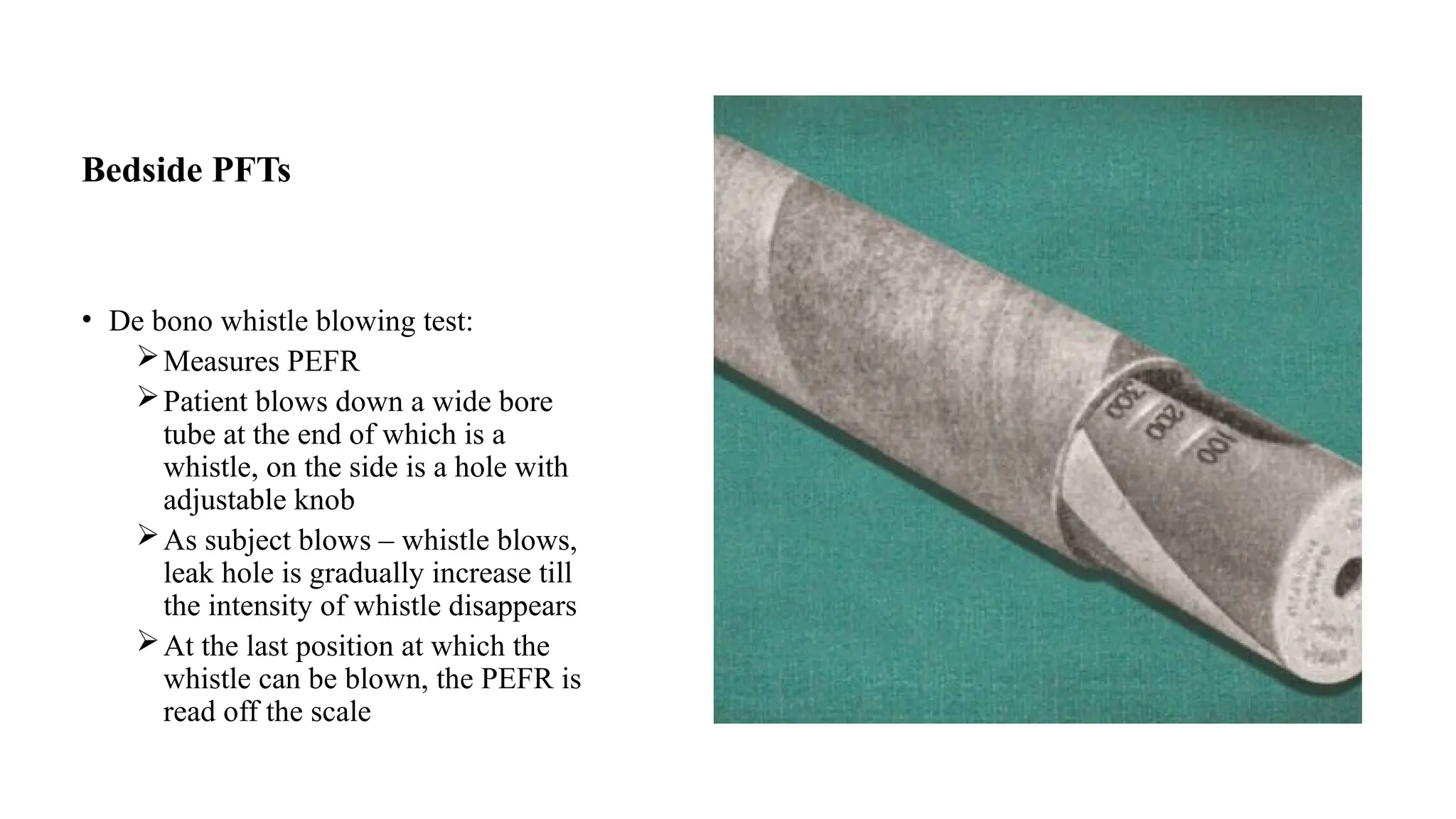
• Debono whistle blowing test:
Measures PEFR
Patient blows down a wide bore
tube at the end of which is a
whistle, on the side is a hole with
adjustable knob
As subject blows – whistle blows,
leak hole is gradually increase till
the intensity of whistle disappears
At the last position at which the
whistle can be blown, the PEFR is
read off the scale
19.
Bedside PFTs
• Primaryfunction of cardiorespiratory system is transport of O2 and Co2.
• O2 delivery=cardiac output x arterialo2 content Cao2
• CaO2 = 1.34 x sa02 x Hb + 0.003 x paO2
• 1.34 ml/g is the o2 binding capacity of Hb(hufner constant)
• Sa02 is o2 saturation of Hb in arterial blood
• 0.003is solubility of O2 in blood (ml/100 ml/mmhg)
• PaO2 is arterial partial pressure of O2.
20.
PULSE OXIMETRY
• FunctionalSaO2 =O2 Hb /O2 Hb +deO2Hb *100%
• Fractional SaO2=O2Hb/O2Hb +DeOxHb +CoHb+ SHb+ MetHb*100%
• Pulse oximetry is a fifth vital sign
• It is non-invasive method of measuring Hb saturation with O2.
21.
PULSE OXIMETRY
• Principle:
•Oximetry is an application of Beer Lambert Law
• Transmission of light through a solution to the concentration of solute in the
solution
• Itrans = I Inc e-
• Itrans = Intensity of transmitted light
• I Inc = Intensity of Incident light
• e = base of natural logarithm
• D = distance of light transmitted through the solution
• C = concentration of the solute
• = extinction coefficient of the solute
22.
Pulse Oximetry
• Continuousassessment of functional SaO2 –based on pulse oximetry denoted as
spO2
Functioning mechanism:
• Pulsality of arterial blood flow provide an estimate of SaO2 by differential light
absorption by arterial blood from light absorption from other components.
• Light absorption by tissues:
a)pulsatile component (AC-alternating current)
b)non pulsatile component(DC-direct current)
• Wavelenght used =660nm(great absorption of DeO2 hb) & 940nm (great absorption
of O2 Hb)
• R
23.
Pulse Oximetry
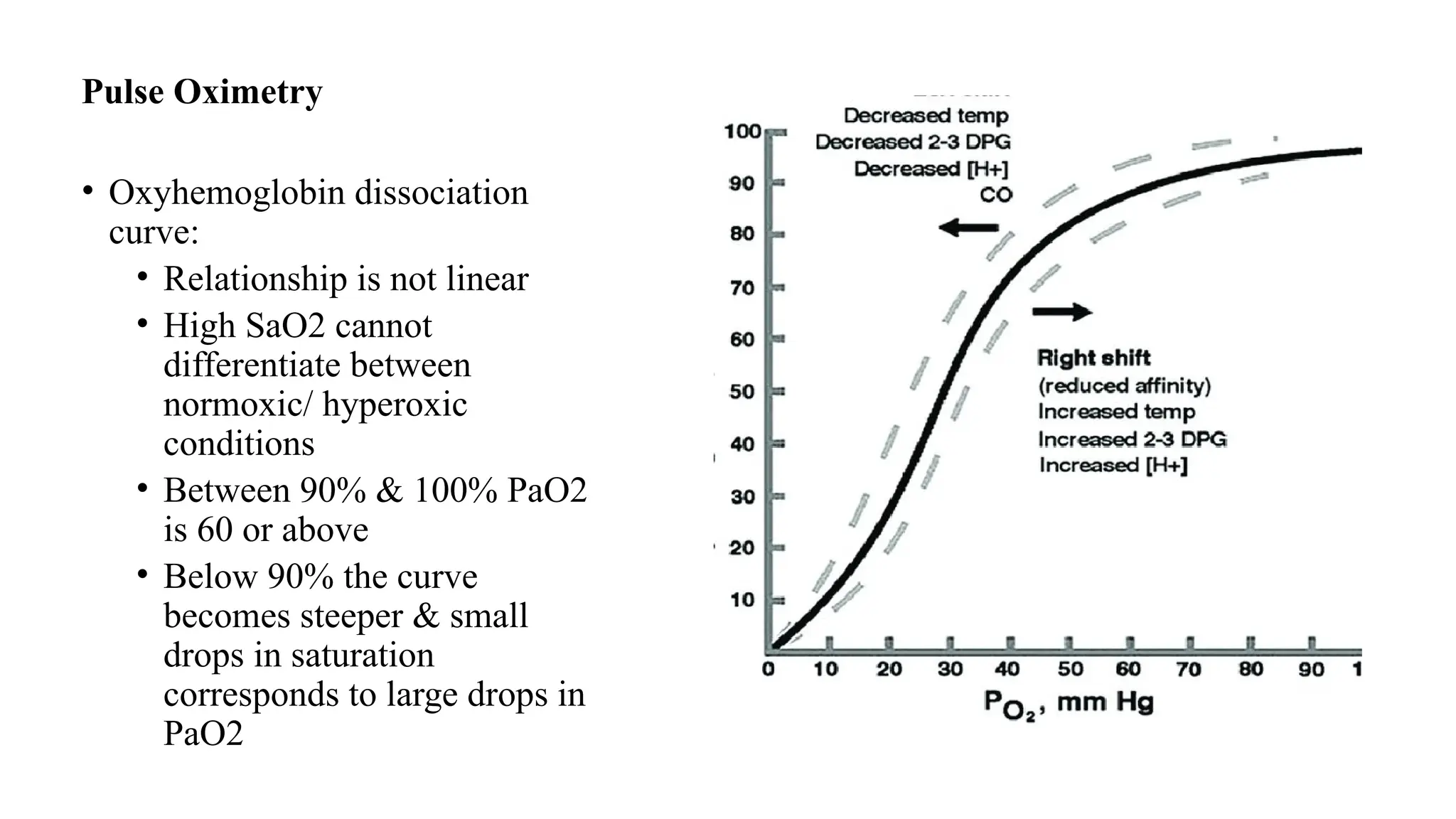
• Oxyhemoglobindissociation
curve:
• Relationship is not linear
• High SaO2 cannot
differentiate between
normoxic/ hyperoxic
conditions
• Between 90% & 100% PaO2
is 60 or above
• Below 90% the curve
becomes steeper & small
drops in saturation
corresponds to large drops in
PaO2
24.
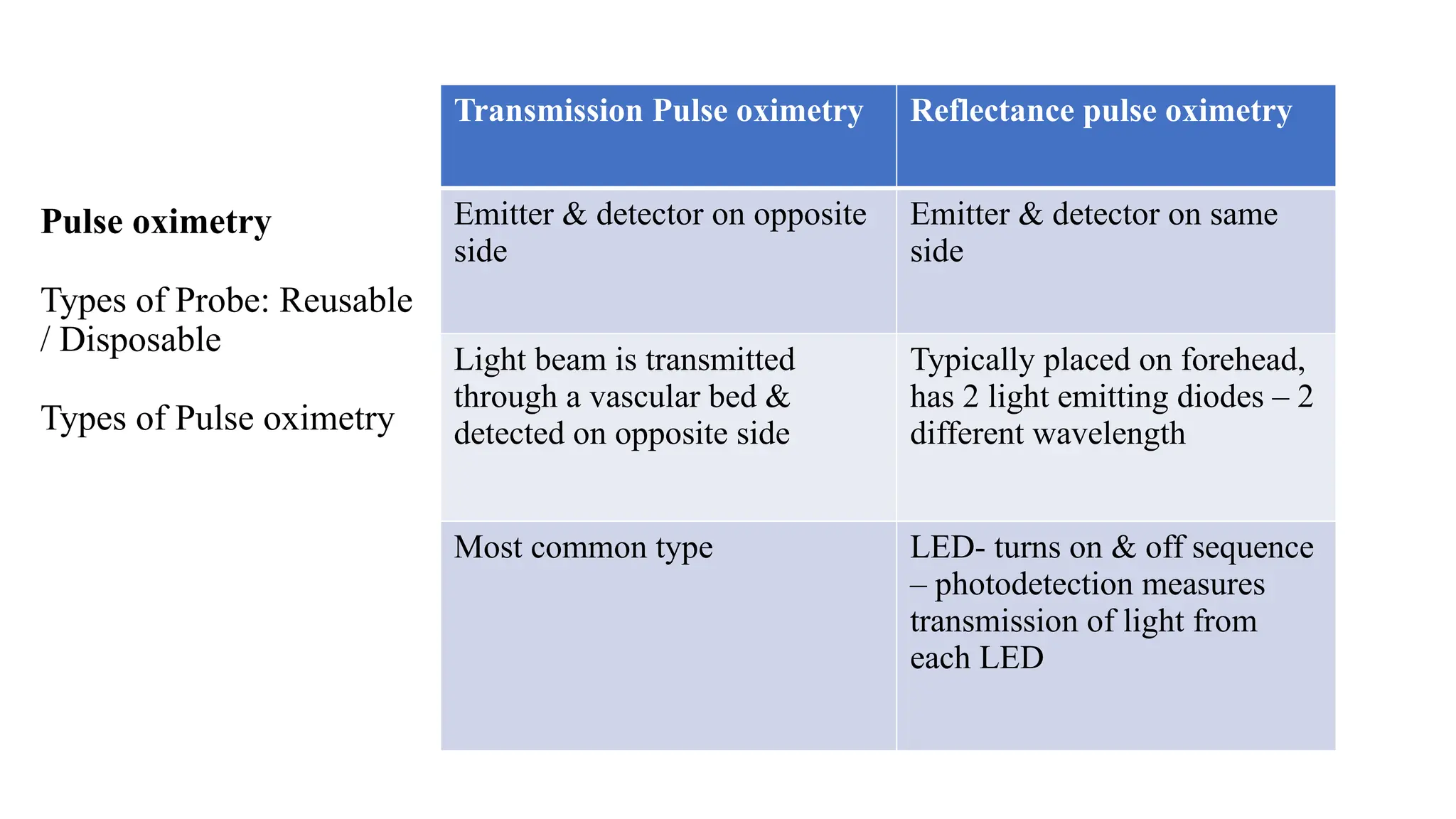
Pulse oximetry
Types ofProbe: Reusable
/ Disposable
Types of Pulse oximetry
Transmission Pulse oximetry Reflectance pulse oximetry
Emitter & detector on opposite
side
Emitter & detector on same
side
Light beam is transmitted
through a vascular bed &
detected on opposite side
Typically placed on forehead,
has 2 light emitting diodes – 2
different wavelength
Most common type LED- turns on & off sequence
– photodetection measures
transmission of light from
each LED
25.
Pulse Oximetry
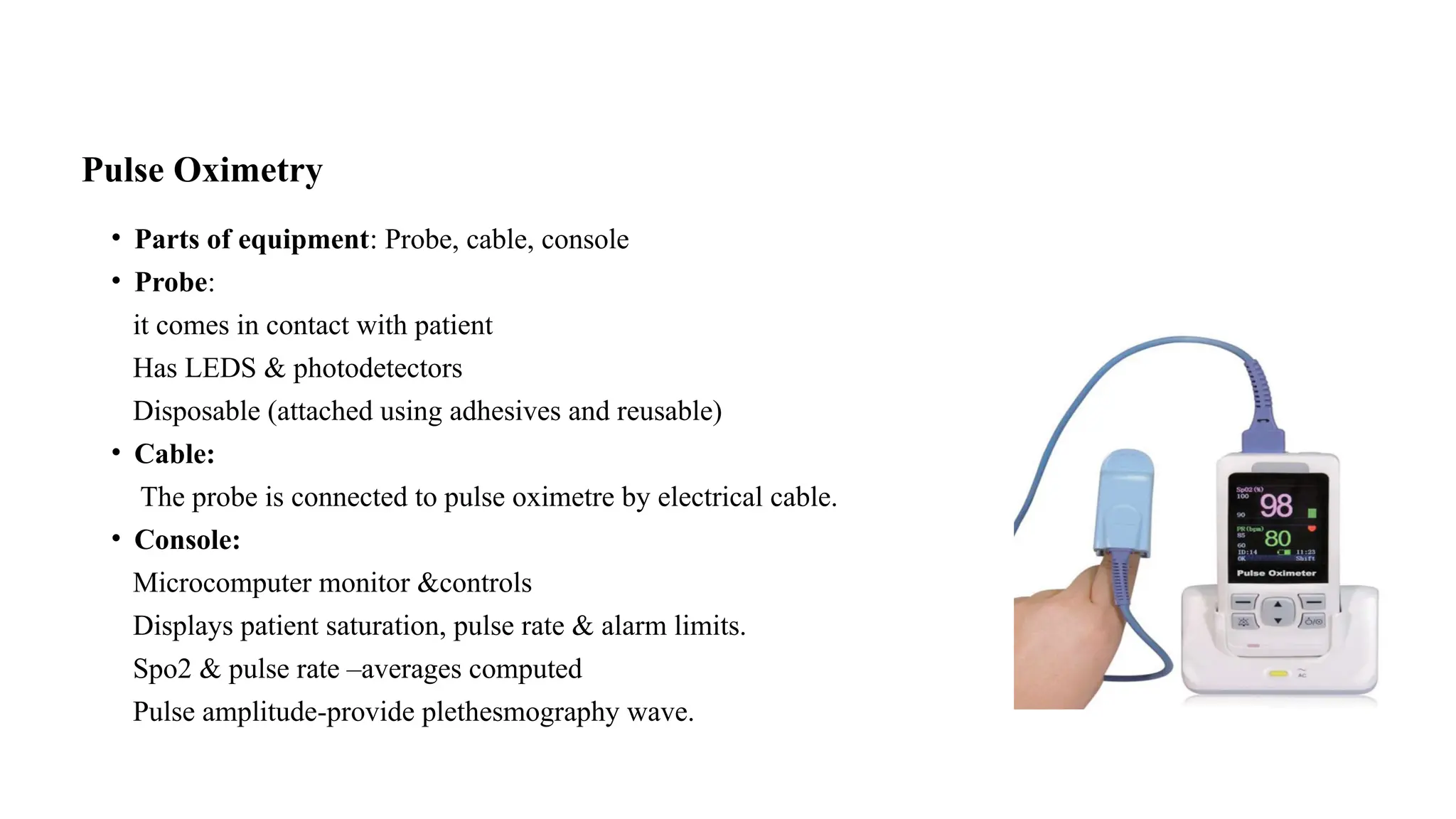
• Partsof equipment: Probe, cable, console
• Probe:
it comes in contact with patient
Has LEDS & photodetectors
Disposable (attached using adhesives and reusable)
• Cable:
The probe is connected to pulse oximetre by electrical cable.
• Console:
Microcomputer monitor &controls
Displays patient saturation, pulse rate & alarm limits.
Spo2 & pulse rate –averages computed
Pulse amplitude-provide plethesmography wave.
26.
Pulse oximetry
Sites:
Finger:
• Mcsite. Failure rate is less and accuracy is better.
• Disadvantage : Detection of desaturation and resaturation is slower.
Toe:
• Alternate site
• Reliable signal in patients with epidural block –increase in amplitude means successful block.
Nose:
• Recommended in hypothermic, hypotension, infusion of vasoconstrictor drugs
• In trendelenberg position-nasal congestion occurs which gives falsely low saturation values.
27.
23/02/2025 Dr VinodKumar 27
Ear:
• Immune to vasoconstrictive effects.
• Gives erroneous reading in steep head down & tricuspid incompetence
Tongue/Esophagus/Forehead:
• Reflectance pulse oximetry is used.
28.
Pulse Oximetry
• Applicationsof Pulse Oximeter:
• Anesthesiology areas
• Post anesthetic care unit
• Transport: during transport from OT to PAC, other intra hospital areas
• Out of hospital use: while shifting the patient in ambulance
• Controlling Oxygen administration:
• lowest safe O2 flow
• Monitoring peripheral circulation:
• Monitoring O2 saturation – shoulder arthroscopy
• To detect brachial artery compression
• Not helpful in detecting compartment syndrome as diminution of arterial pulse is late sign
• Mediastinoscopy: compression of brachiocephalic artery & aortic arch between
mediastinoscope & sternum
29.
• Limitations:
• Itwill not provide information about tissue oxygenation
• Failure to determine O2 saturation: ASA- 3,4 or 5, hypothermia, hypotension, chronic
kidney failure, low hematocrit & motion
• Poor perfusion: loss or diminution of peripheral pulse – pulse oximetry cannot detect pulse
• Difficulty in detecting high O2 partial pressures i.e above 90mmHg
• SPO2 values underestimates SaO2 in anemic patients with true hypoxemia.
• Erratic performance with dysrhythmias
• Nail Polish ( Dark blue, purple, black interferes)
• Dyes: Methylene blue decrease SPO2 65%, indigo carmine & indocyanine green also
decreases
• Methyl Hb: absorbs light @ 660nm & 940nm, R=1, corresponds to SpO2 – 85%- no matter
the value of SaO2
• CO poisoning – falsely elevated