Downloaded 1,387 times


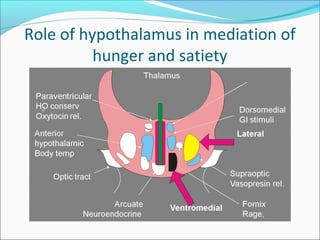
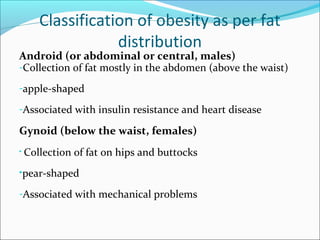
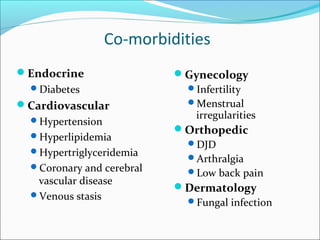

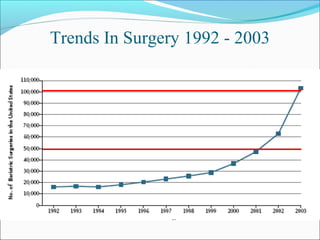
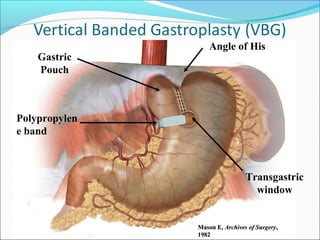

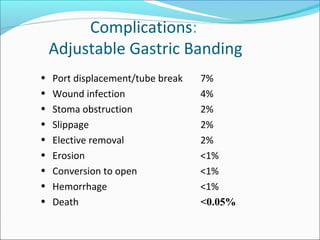
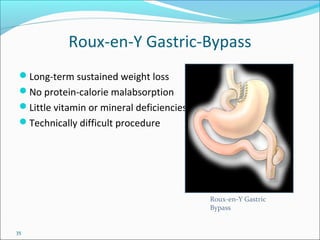
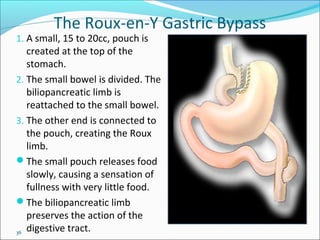
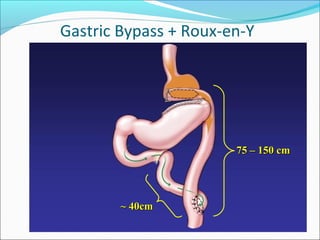
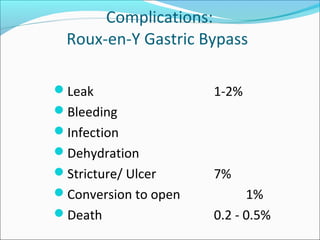
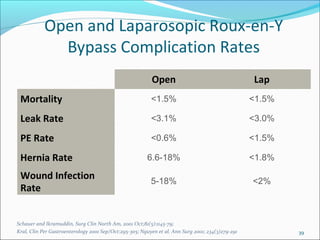
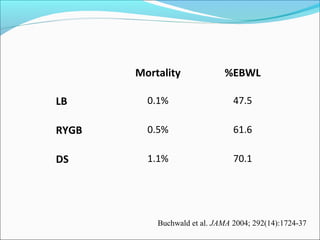

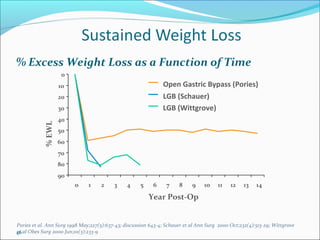

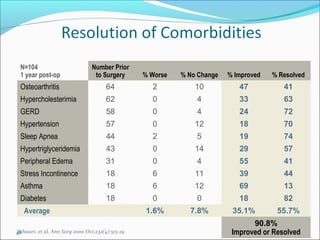
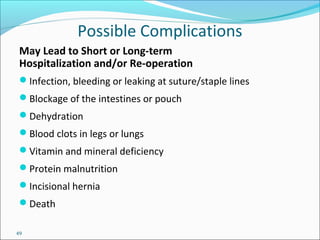






This document provides information about obesity, including definitions, classifications, causes, comorbidities, and treatments. It discusses: - Definitions of obesity based on body mass index (BMI) and classifications of overweight and obesity. - Causes of obesity including genetic, hormonal, environmental, and behavioral factors. - Common obesity-related health conditions or comorbidities such as diabetes, heart disease, sleep apnea, cancer, and arthritis. - Treatment options for obesity including lifestyle changes, medications, bariatric surgery procedures like gastric bypass and banding, and their risks and effectiveness. Bariatric surgery can result in significant and long-term weight loss and improvement of comorbidities.























































































