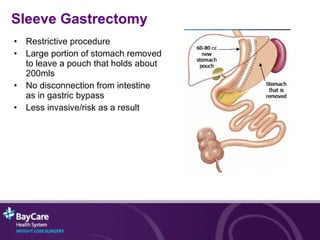
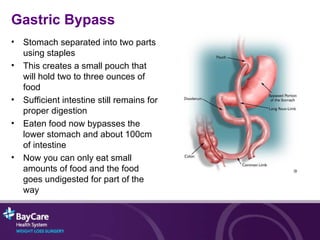
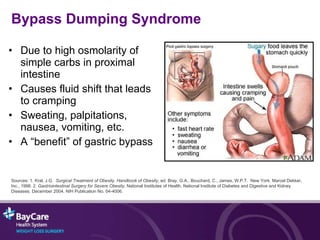
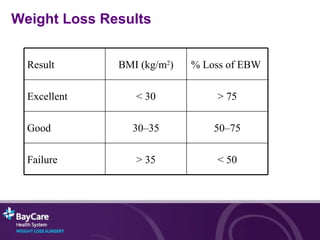
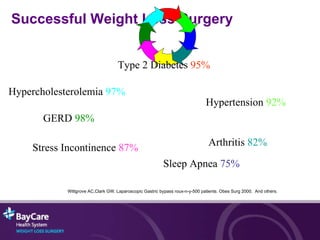
The document summarizes information presented at a weight loss information session. It discusses obesity, weight loss surgery options including gastric bypass, gastric banding and sleeve gastrectomy, the process of weight loss surgery, expected results including improved health outcomes and weight loss, and next steps a patient should take to pursue surgery.





























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















