Downloaded 382 times

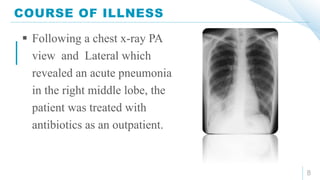




This document describes a case of pneumonia in a 68-year-old male smoker who presented with cough, fever, and chest pain. On examination, he appeared tired and underweight with decreased breath sounds on the right lung. A chest x-ray showed right middle lobe pneumonia. He was treated as an outpatient with antibiotics, but a follow-up x-ray found a right hilar mass and sputum testing demonstrated atypical cells, indicating a more serious condition. The document provides answers to questions about identifying problems in the history, significant physical findings, likely causative organisms, how the specific diagnosis is established, appropriate treatment, and expected duration of treatment.























































































