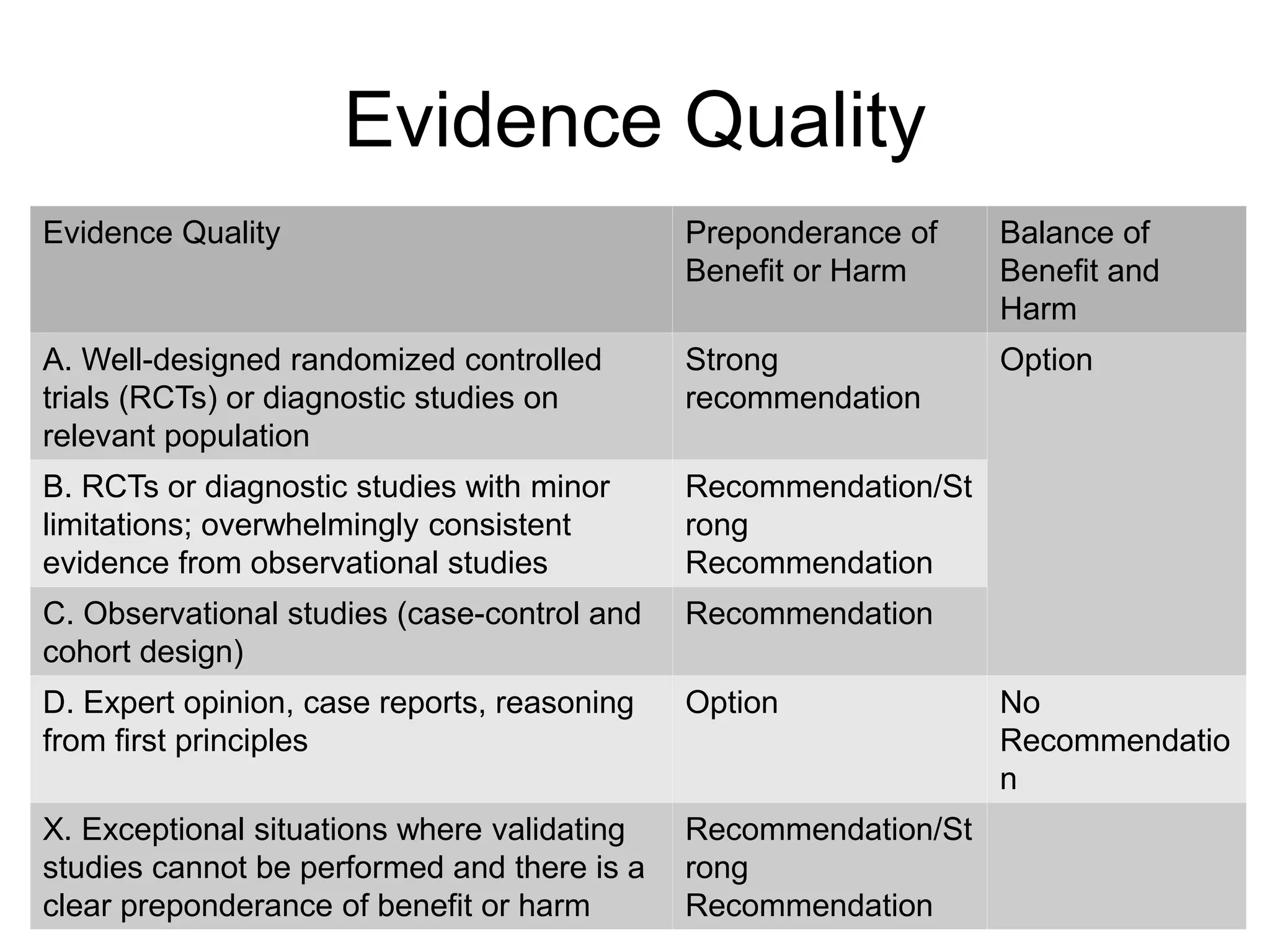
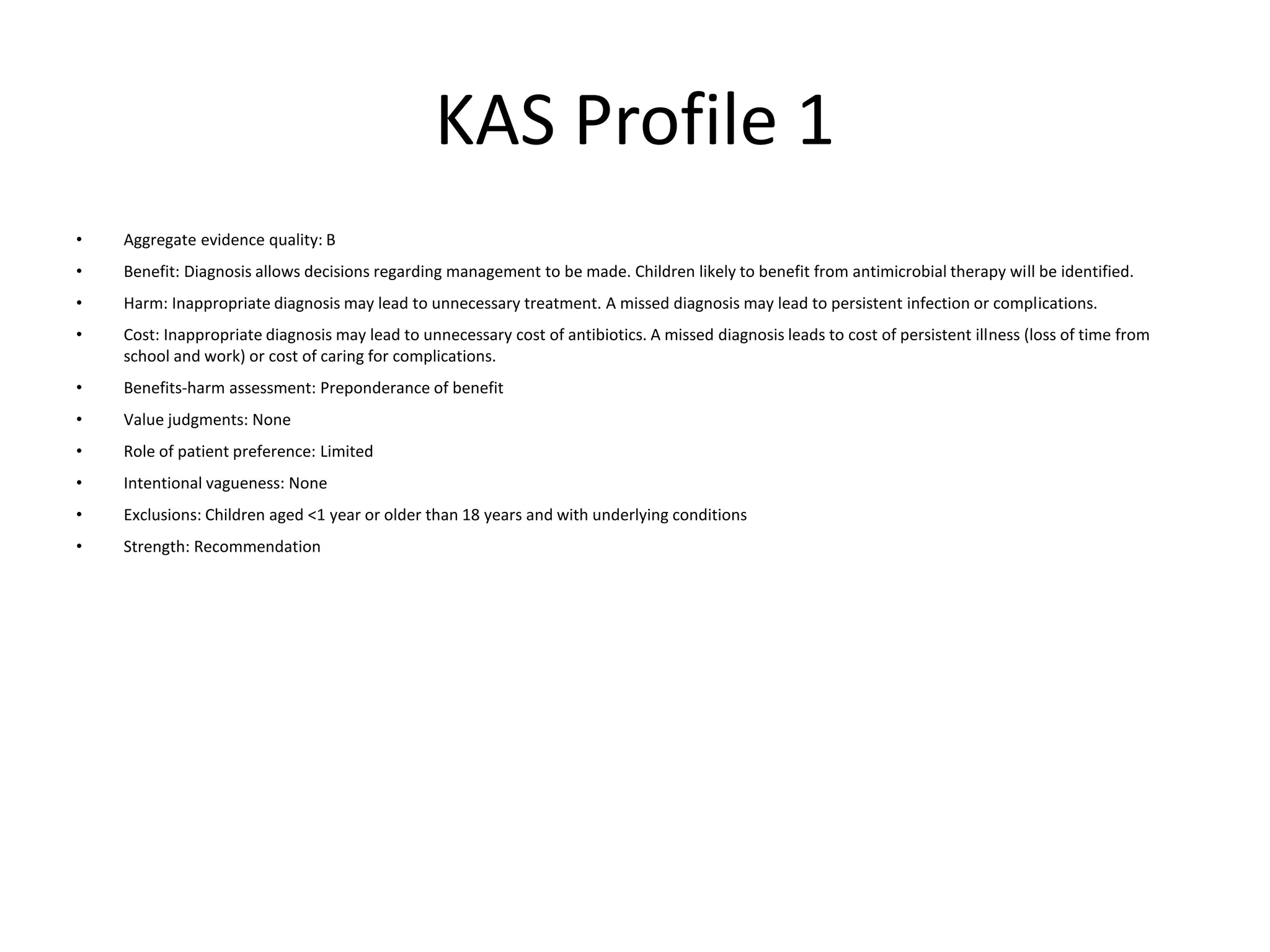
1. The document discusses the pathogenesis and diagnosis of acute bacterial sinusitis in children, including defining the typical bacterial causes, the role of prior viral infections in enabling bacterial overgrowth, and guidelines for diagnosing based on symptom duration and severity.
2. Imaging studies like CT scans are not recommended to distinguish between viral and bacterial infections but are recommended if complications like orbital or central nervous system issues are suspected.
3. The guidelines recommend prescribing antibiotics for severe or worsening cases but allow either antibiotics or additional observation for persistent cases lasting over 10 days without improvement.





![Key Action Statement 1
• Clinician should make a presumptive diagnosis of acute bacterial sinusitis when a child with an acute upper
respiratory tract infection (URI) presents with the following:
• Persistent illness (i.e., nasal discharge [of any quality] or daytime cough or both lasting more than 10 days
without improvement)
• OR
• Worsening course (i.e., worsening or new onset of nasal discharge, daytime cough, or fever after initial
improvement)
• OR
• Severe onset (i.e., concurrent fever [temperature ≥39°C/102.2°F] and purulent nasal discharge for at least
3 consecutive days)
• (Evidence Quality: Grade B; Recommendation)](https://image.slidesharecdn.com/acutebacterialsinusitis-190830225324/75/Acute-bacterial-sinusitis-11-2048.jpg)
![Key Action Statement 2.A
• Clinicians should not obtain imaging studies
(plain films, contrast-enhanced computed
tomography [CT], magnetic resonance imaging
[MRI], or ultrasonography) to distinguish acute
bacterial sinusitis from viral URI (Evidence
Quality: Grade B; Strong Recommendation).](https://image.slidesharecdn.com/acutebacterialsinusitis-190830225324/75/Acute-bacterial-sinusitis-13-2048.jpg)