Downloaded 545 times

![• Autistic Disorder Dr.Padmesh. V
• PROGNOSIS.
• Better prognosis:
• Higher intelligence, functional speech, and less bizarre symptoms and
behavior better prognosis. [may grow up to live self-sufficient,
employed life in community.(though isolated) ]
• Early intensive therapy
• Bad prognosis:
• Many have bad prognosis, & remain dependent on family for their
everyday needs.
• Delayed diagnosis leads to poor outcome.](https://image.slidesharecdn.com/autism-dr-padmesh-111204090259-phpapp02/85/Autism-Dr-Padmesh-43-320.jpg)



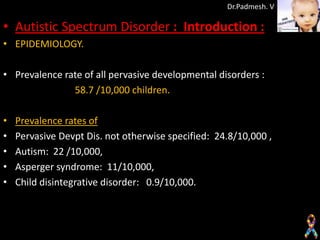
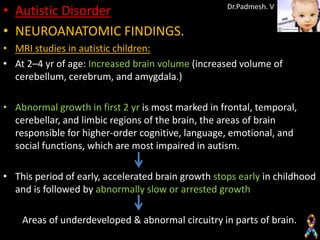
The document discusses autism spectrum disorder and provides information on autistic disorder. It notes that the prevalence of pervasive developmental disorders is 58.7 per 10,000 children. Autistic disorder is a neurodevelopmental disorder diagnosed before age 3 that involves impairments in social interaction, communication, and imagination/play. The cause is unknown but has a strong genetic component. Diagnostic criteria and clinical features of autistic disorder are provided.




























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








