




![screening test for autism (such as the
Checklist for Autism in Toddlers [CHAT]
or the Autism Screening Questionnaire).
genetic testing
complete physical
examination
nervous system (neurologic)
examination.](https://image.slidesharecdn.com/autismppt-130826013452-phpapp02/85/AUTISM-ppt-43-320.jpg)





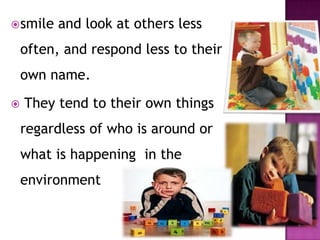
This document provides an overview of autism including: 1. Autism is a developmental disorder appearing in the first 3 years that affects social and communication skills. 2. It was first described by Kanner in 1943 and prevalence is estimated at 2-6 per 1000 individuals. 3. Prognosis depends on severity but proper therapy can help individuals improve socialization and live independently.