Downloaded 67 times

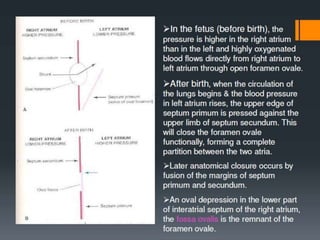

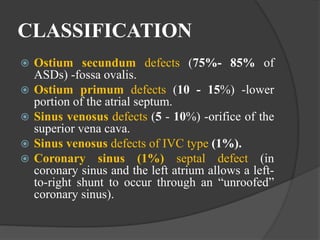
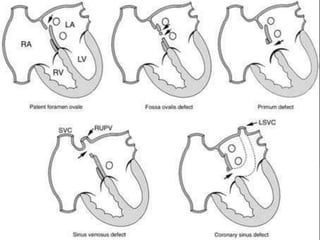
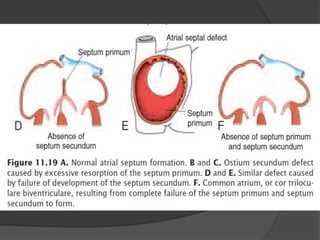
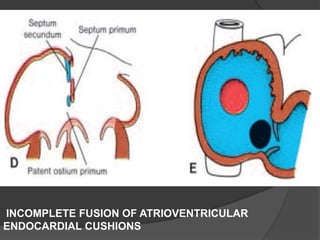
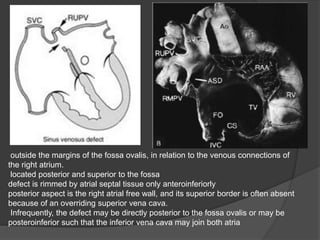
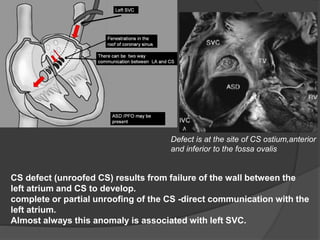






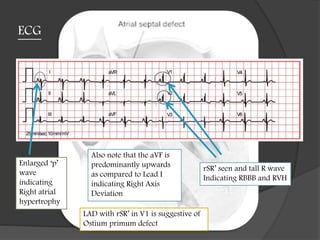

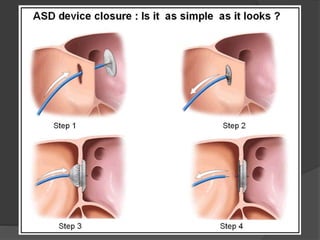

1. Atrial septal defects can be classified into four main types based on their location: ostium secundum, ostium primum, sinus venosus, and coronary sinus defects. 2. Ostium secundum defects, which account for 75-85% of ASDs, involve a defect in the fossa ovalis. Ostium primum defects involve the lower portion of the atrial septum. 3. The likelihood of spontaneous closure of an ASD depends on its size, with defects larger than 8-10 mm being less likely to close compared to smaller defects.





















































































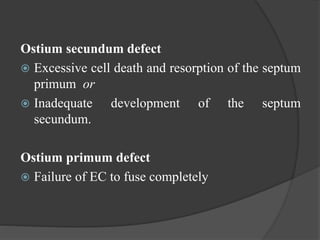
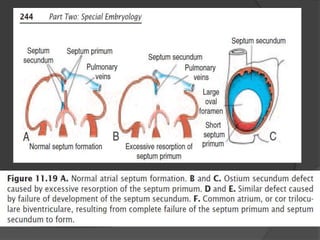
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

