


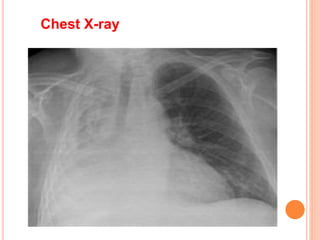









Atelectasis is a lung condition where alveoli collapse due to excess mucus blocking airways. It can be acute, such as during anesthesia, or chronic due to obstructive disorders. Symptoms include cough, sputum, fever, and dyspnea. Diagnosis involves chest x-ray, CT scan, and bronchoscopy showing collapsed lung areas. Treatment focuses on clearing secretions through coughing, deep breathing, and chest physiotherapy to reopen airways and prevent further collapse.