Download to read offline







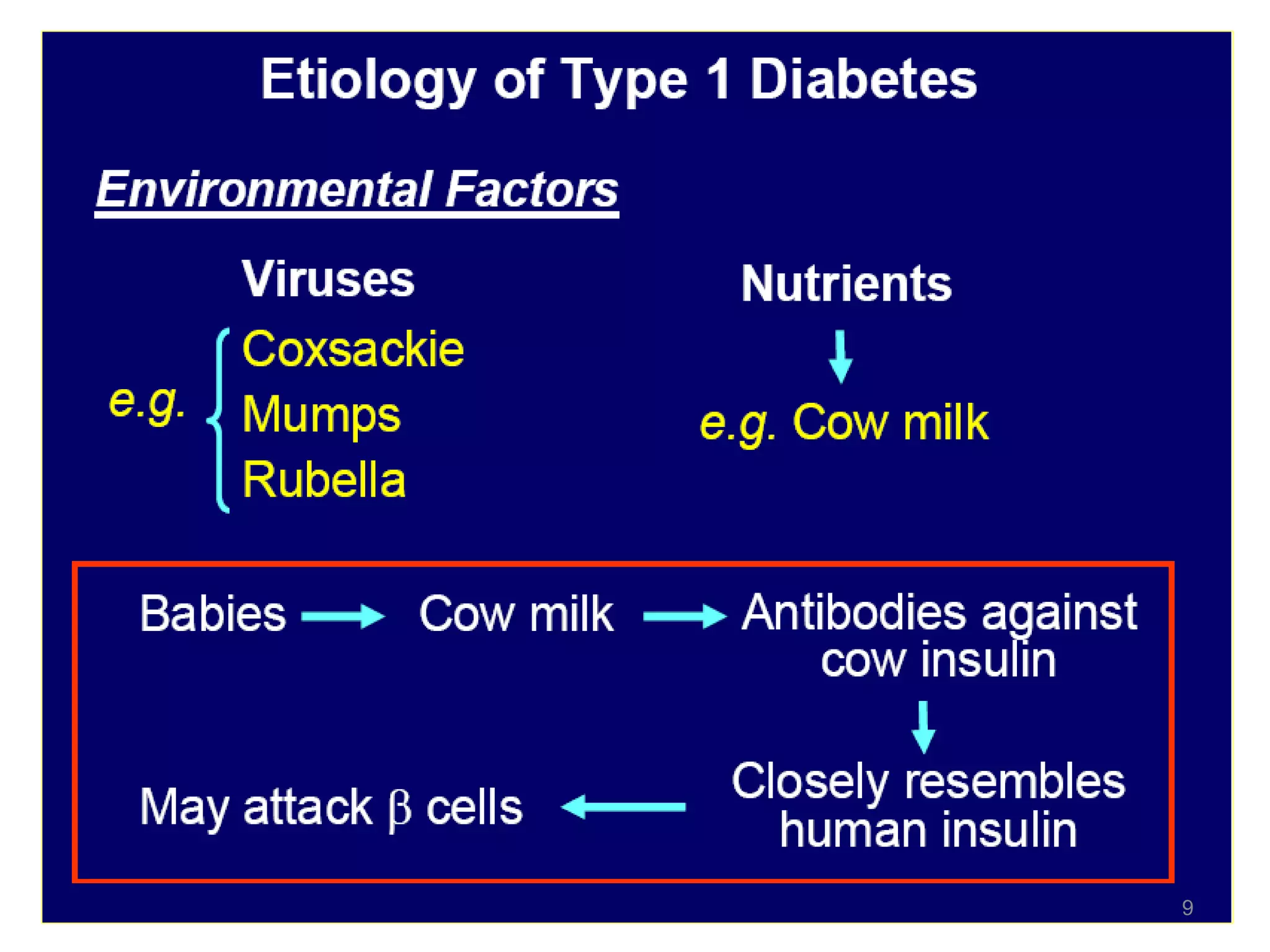










The document discusses diabetes mellitus (DM), which is characterized by high blood glucose levels due to defects in insulin production or action. There are two main types of DM: Type 1 is an autoimmune disease where the body destroys insulin-producing cells, while Type 2 is associated with obesity and aging and results from insulin resistance and relative insulin deficiency. Gestational diabetes occurs during pregnancy and increases risk of future Type 2 DM. Other types include genetic disorders. The prevalence of DM, especially Type 2, is increasing worldwide due to rising obesity and physical inactivity.





























































![DM lecture for c1 [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/dmlectureforc1autosaved-220720190831-86418752-thumbnail.jpg?width=640&height=640&fit=bounds)





















![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)


















