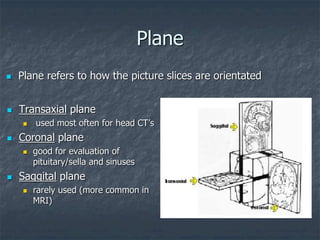
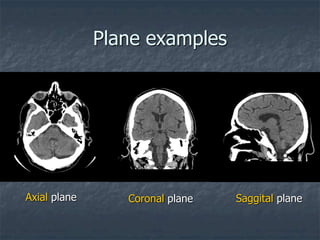
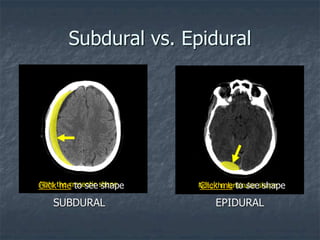
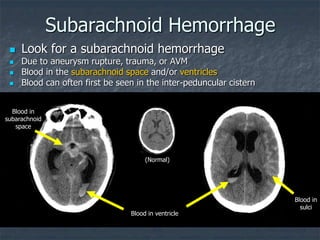
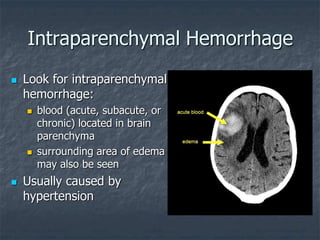
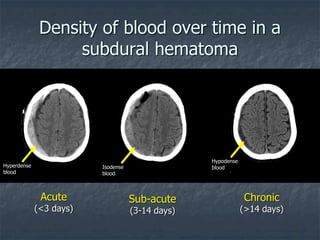
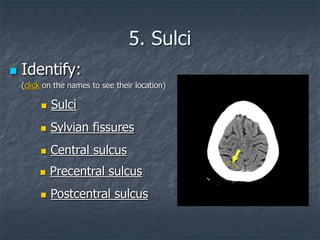
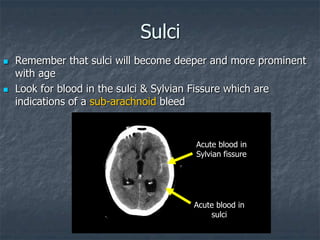
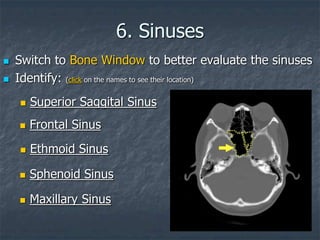
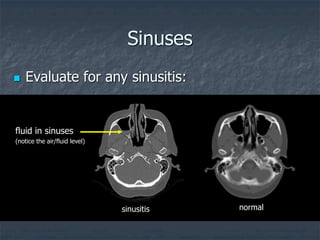
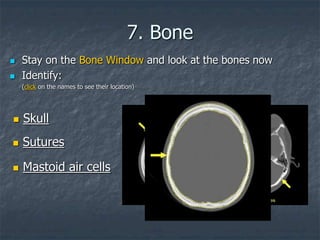
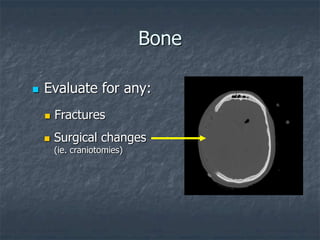
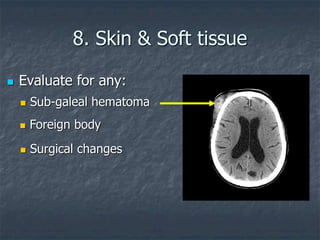
This document provides an overview of how to systematically analyze a head CT scan. It begins with identifying basic scan details and checking for previous studies. It then reviews CT fundamentals like Hounsfield units and image planes. The document outlines an approach of analyzing midline structures, ventricles, cisterns, brain parenchyma, sulci, sinuses, and bones. It provides examples of common abnormalities and how to identify acute vs. chronic hemorrhages. The goal is to familiarize readers with head CT anatomy and classic abnormalities.