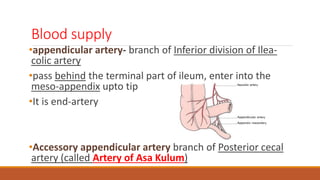
The appendix is a small tube located near the cecum. It develops in the 8th week of gestation and rotates 270 degrees before settling in the right iliac fossa. The appendix has numerous lymphoid follicles and goblet cells but its function in adults is unknown. Acute appendicitis presents with migratory abdominal pain, anorexia, nausea and tenderness near the right iliac fossa. Diagnosis is suggested by elevated white blood cell count and confirmed by CT scan or ultrasound showing a swollen, non-compressible appendix. Treatment is surgical removal of the appendix (appendectomy). Complications can include abscess, perforation or gangrene if not treated promptly.










![LAB
L – Leukocytosis - 2
S – Left shift [progenitor WBC
cell in periphery] - 1](https://image.slidesharecdn.com/appendicitis-150417141903-conversion-gate01/85/Appendicitis-20-320.jpg)