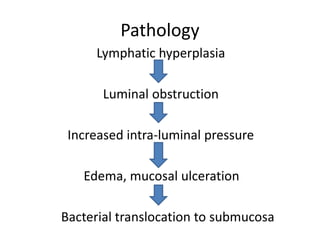
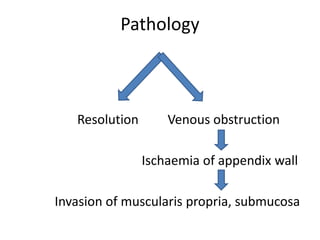
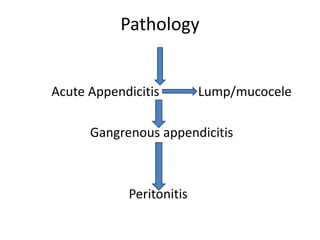
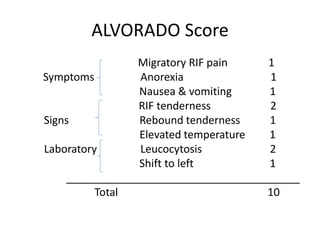
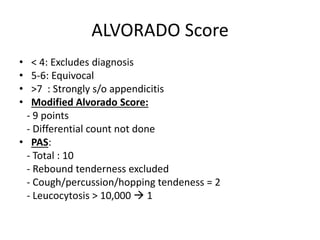
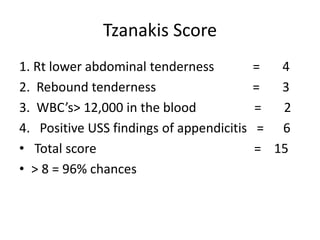
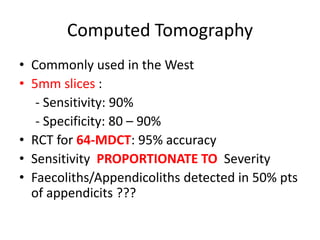
The document discusses acute appendicitis, providing details on the anatomy of the appendix, etiology, pathology, clinical features, differential diagnosis, investigations including scoring systems like the Alvarado score, treatment including appendicectomy, and complications. Acute appendicitis is most commonly caused by obstruction of the appendix lumen, leading to increased intra-luminal pressure, edema, and bacterial invasion. Clinical diagnosis is important but imaging modalities like CT scans can help when clinical signs are unclear or atypical.

































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)













