DEFINITION
• APPENDIX VERMIFORM:The appendix is a
finger-shaped pouch that sticks out from the
colon on the lower right side of the abdomen.
• APPENDICITIS: is the inflammation of the
appendix
4.
HISTORIQUE PERSPECTIVE
• 1736:The first appendectomy was
performed by AMYAND
• 1886: The word “appendicitis” was
introduced by REGINALD FITZ
• 1899: MC BURNEY, described the clinical
manifestation of early appendicitis,
including the point of maximum tenderness
in the R.I.F.
5.
INTRODUCTION
• Appendicitis isone of the most common cause of
acute abdomen world wide with a life risk 8.6 %
in males and 6.9% in females
• For over a century, open appendectomy was the
only standard treatment for appendicitis.
• Contemporary management of appendicitis is
laparoscopic appendectomy
• treat uncomplicated appendicitis nonoperatively
with antibiotics alone.
6.
EMBRYOLOGY
• First becomesvisible in the eighth week of
embryologic development as a protuberance
off the terminal portion of the cecum.
• During both antenatal and postnatal
development, the growth rate of the cecum
exceeds that of the appendix, displacing the
appendix medially toward the ileocecal valve
7.
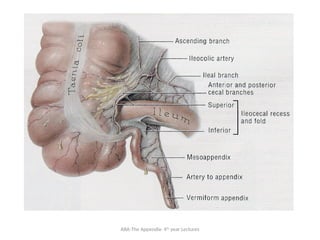
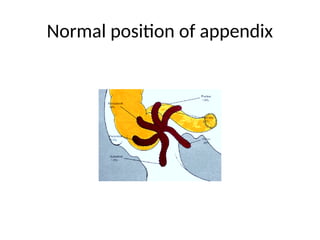
ANATOMY
• Small blind-ending,muscular tube at the meeting
point of the 3 taenia coli, just distal to the I. C.
junction.
• located in the right lower section of the abdomen.
• The average length is 7.5-10cm(2-20cm)
• The normal lumen (< 6mm): , irregular, being
encroached by multiple longitudinal folds of M.M.
• Blood supply: app. A. I. C. A
• Venous drainage: app. V. I.C.V.
• Lymphatic vessels: 4,6,more I.Caecal. L.Ns.
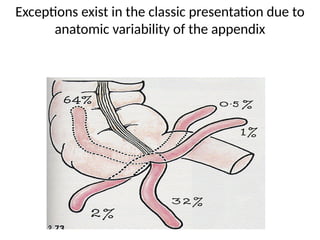
Exceptions exist inthe classic presentation due to
anatomic variability of the appendix
11.
EPIDEMIOLOGY
• Most commonacute surgical condition of the
abdomen
• Peak incidence in early adulthood
• 7-10% of population develop acute appendicitis
• More in males 1.3-2 : 1
• Mortality is 0.3to 0.85% but in elderly it is >20%
• Despite newer imaging techniques, acute
appendicitis can be very difficult to diagnose.
etio
• STRICTURE (fibrosis,Crohn’s disease )
• FOREIGN BODY
• NEOPLASM: ca. of caecum, carcinoid synd.
• PARASITES:oxyuris vermicularis (pin warm
• INFECTION:
- bacterial proliferation within the appendix
- mixed growth of aerobic & anaerobic
(E.coli 85%, Enterococi 30%, Bacteroids, Cl. Welchi)
• RACE &DIET: The incidence is lowest in societies with high dietary
fiber intake.
• SOCIAL STATUS: more common among the upper & middle class
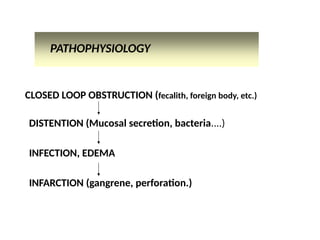
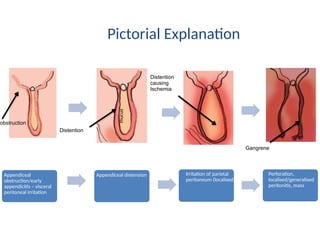
PATHOPHYSIOLOGY
• Acute appendicitisis thought to begin with
obstruction of the lumen
• Obstruction can result from food matter,
adhesions, or lymphoid hyperplasia
• Mucosal secretions continue to increase
intraluminal pressure
• Eventually the pressure exceeds capillary
perfusion pressure and venous and lymphatic
drainage are obstructed.
17.
PATHOPHYSIOLOGY…cont.
• With vascularcompromise, epithelial mucosa
breakdown and bacterial invasion by bowel
flora occurs.
• Increased pressure also leads to arterial stasis
and tissue infarction
• End result is perforation and spillage of
infected appendiceal contents into the
peritoneum
PATHOPHYSIOLOGY
• NONE OBSTRUCTIVEAPPENDICITIS
• Inflammation start from the mucosa membrane
but no obstruction, less distention but if serosa is
involved patient develop local peritonitis and
hence pain in the RIF
• This inflammation can lead to: suppuration, or
gangrene, perforation or resolution
• Subacute, recurrent and chronic peritonitis
results from this none obstructive type
EPIDEMIOLOGY
• Incidence ofappendicitis is higher in developed
countries due to consumption of low fiber diet
• Incidence of appendicitis is lower in cultures
with higher fiber diet is intake
• Peak incidence in early adulthood
• 7-10% of population develop acute appendicitis
• More in males 1.3-2 : 1
22.
Clinical Manifestations
• PAIN-dull, vague, Epigastric or peri-umblical, for 6-12 hrs. then
• shifts to the right lower quadrant.
• ANOREXIA ( constant c.feature > 90%, children)
• NAUSEA and
• INFREQUENT VOMİTING (1or 2 episodes,75%).
• Constipation, occasionally diarrhea
• Often, H.O. similar discomfort that settled spontaneousl
• Family H. ( up to 1/3rd
of children)
23.
Atypical presentation:
• Pain, predominantly somatic/ visceral,&
poorly localized (elderly).
• R.L.Q.
• L.L.Q long app., infl. tip in the L.L.Q.
• Flank/ back: retroperitoneal app.
• Supra-pubic: pelvic
24.
Clinical SIGNS
• Appearsuncomfortable,
• Activity: quiet
• Position: frequently shifting position(flexed hip)
• Vital signs:
In the 1st
6 hrs., rare alteration in temp. & P.R. (normal)
• Slight pyrexia (37.2- 37.7°C ) + P.R. to 80 or 90/min.
• 39-40°C: perforation/ gangrene, then if shock ensue.
• > 40°C- abscess, septicemia, infection in C.N.S, Lungs,
U.T.I.
25.
Clinical SIGNS
• Muscleguarding
• Localized tenderness in the R.L.Q. (Maximal at the Mc
Burney’s p.)
• Rebound tenderness
• Cutaneous hyperasthesia
• Rovsing Sign
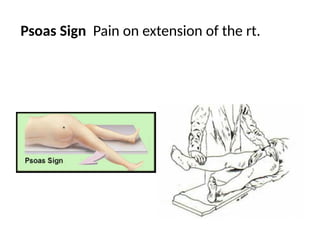
• Iliopsoas Sign
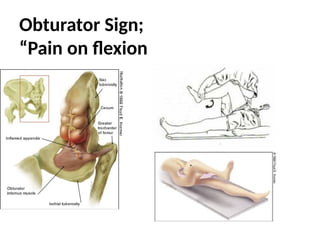
• Obturator Sign
• Rectal exam. : extreme anterior pelvic tenderness
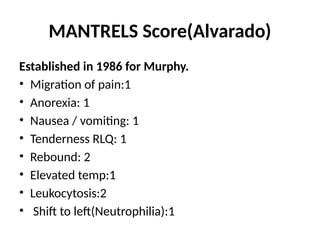
MANTRELS Score(Alvarado)
Established in1986 for Murphy.
• Migration of pain:1
• Anorexia: 1
• Nausea / vomiting: 1
• Tenderness RLQ: 1
• Rebound: 2
• Elevated temp:1
• Leukocytosis:2
• Shift to left(Neutrophilia):1
29.
ALVARADO SCORE
Total score:10
Score8-10: acute appendicitis=> Appendectomy
Score 6-8: possibility of appendicitis(need for
Abd USS or CT Scan for confirmation
Score <6: less likely appendicitis
HIGH RISK PATIENTS,CONT'D
• Pregnancy
– Most common surgical emergency in pregnancy
– Mortality rate if missed = 2 % for mother, up to 35
% for fetus
– WBC elevated in pregnancy
– Appendix changes location
32.
HIGH RISK PATIENTS,CONT'D.
• Pediatrics
– Most common surgical disorder in kids
– Accounts for 5 % of abd. pain visits
– Up to 50 % initially misdiagnosed
• < 2 yrs. : perforation rate approaches 100 %
• 3 to 5 yrs. = 71 %
• 6 to 10 yrs. = 40 %
– Most common misdiagnosis is AGE
– Sequence of pain and vomiting may be helpful
– Localized tenderness not a feature of AGE
33.
HIGH RISK PATIENTS,CONT'D.
• Elderly
– Vital signs and exam may not reflect severity
– > age 60 : only 5 to 10 % diagnosed without delay
– Perforation rate = 46 to 83 %
– RLQ tenderness absent in 23 %
– N/V, anorexia less common
– Leukocytosis less pronounced
– Only 20 % classic presentation
34.
HIGH RISK PATIENTS
•Ovulating women
– PID, TOA, ovarian cyst rupture can mimic
appendicitis
– Look for cervical motion tenderness, adnexal
tenderness, history of STD’s
– Can have CMT with pelvic appendix
35.
HIGH RISK PATIENTS,CONT'D.
Immunocompromised
– HIV, chronic steroids, sickle cell anemia,
chemotherapy, DM, dialysis
– Increased risk of complications and misdiagnosis
• Inflammatory response decreased
LABORATORY STUDIES
• FBC
–75 to 85 % have elevated WBC, but it is
nonspecific
– WBC normal in 80 % in the first 24 hrs.
– WBC usually 12 to 18,000 in appendicitis
• Chemistry panel
– May help with diagnosis of dehydration
•
38.
IMAGING STUDIES
• Plainfilms
– Low sensitivity and specificity
– Appendicolith specific, but seen in only 2 %
– May see local air-fluid levels, psoas obliteration, soft tissue
mass, gas in appendix : all nonspecific
• Ultrasound
– 75 to 90 % sensitive, 86 to 100 % specific
– Noninvasive, low cost, but operator-dependent
– Good for diagnosing GYN disorders
CT SCAN
– Earlystudies showed low yield, but helical CT much more
accurate
– Sensitivity 97 to 100 %, specificity 95 % (similar no matter
what type or whether contrast is used)
– Often shows alternative diagnosis
– More expensive, radiation exposure
Criteria for appendicitis :
• Diameter > 6 mm
• Failure to completely fill with contrast or air
• Appendicolith
• Wall thickening or enhancement
– Other contributory signs include fat stranding, fluid,
inflammatory mass, adenopathy
TREATMENT
The goal ofthe surgical approach
An early diagnosis with resection of an acutely
inflamed appendix prior to perforation,
A minimum of negative appendectomies.
• Appendectomy is the standard of care
• Patients should be NPO, given IVF, and preoperative
antibiotics
• Antibiotics are most effective when given preoperatively
and they decrease post-op infections and abscess
formation
Problems encountered duringappendectomy
• A normal appendix is found. This demands careful exclusion of other
possible diagnoses, particularly terminal ileitis, Meckel’s diverticulitis and
tubal or ovarian causes in women. It is usual to remove the appendix to
avoid future diagnostic difficulties, even though the appendix is
macroscopically normal
• The appendix cannot be found. The caecum should be mobilised, and the
taeniae coli should be traced to their confluence on the caecum before the
diagnosis of ‘absent appendix’ is made.
• An appendicular tumour is found. Small tumours (under 2.0 cm in diameter)
can be removed by appendicectomy; larger tumours should be treated by a
right hemicolectomy
• An appendicular tumour is found. Small tumours (under 2.0 cm in
diameter) can be removed by appendicectomy;mlarger tumours
should be treated by a right hemicolectomy
46.
Management of anappendix mass
• If an appendix mass is present and the condition of
the patient is satisfactory, the standard treatment is
the conservative
• This strategy is based on the premise that the
inflammatory process is already localised and that
inadvertent surgery is difficult and may be
dangerous.
• Give antibiotics and anti inflammatory and then do
interval appendicectomy after 4 to 6 weeks
OPERATIVE TREATMENT
• TransverseRocky-Davis or the classical McBurney
or midline skin incision is made in the abdomen
over the area of maximal tenderness.
• If purulent or cloudy peritoneal fluid is
encountered, it should be sent for culture and
sensitivity.
• The appendix is identified at the confluence of the
taeniae coli, and the mesoappendix is clamped and
divided.
49.
APPENDECTOMY PROCEDURE
These involve:
-Openappendectomy – an incision is made through the
skin, the underlying tissue and the abdominal wall in
order to access the appendix.
-Laparoscopic (‘keyhole’) appendectomy – this involves
making three small incisions in the abdomen, through
which particular instruments are inserted. A gas is gently
pumped into the abdominal cavity to separate the
abdominal wall from the organs. This makes it easier to
examine the appendix and internal organs.
Appendicular abscess
• Incisionand dreinage
• antibiotics
• Appendicectomy if possible otherwise
• Skin of surgical site should be left opened
• Interval appendicectomy
SUMMURY
• If diagnosisof appendicitis is clear from history and
physical examination no further testing is needed
• When diagnosis of appendicitis is uncertain CT &
ultrasonography may reduce the rate of
perforation and are cost effective
• CT is a better imaging modality for appendicitis
than ultrasonography
• Be aware of other imaging modalities especially
MRI in inconclusive
● ultrasonography or MRI in pregnant females