This document provides information about appendicitis, including:
1. The history of appendicitis diagnosis and treatment from da Vinci's drawings in 1492 to the first successful appendectomy in 1735 to modern laparoscopic procedures.
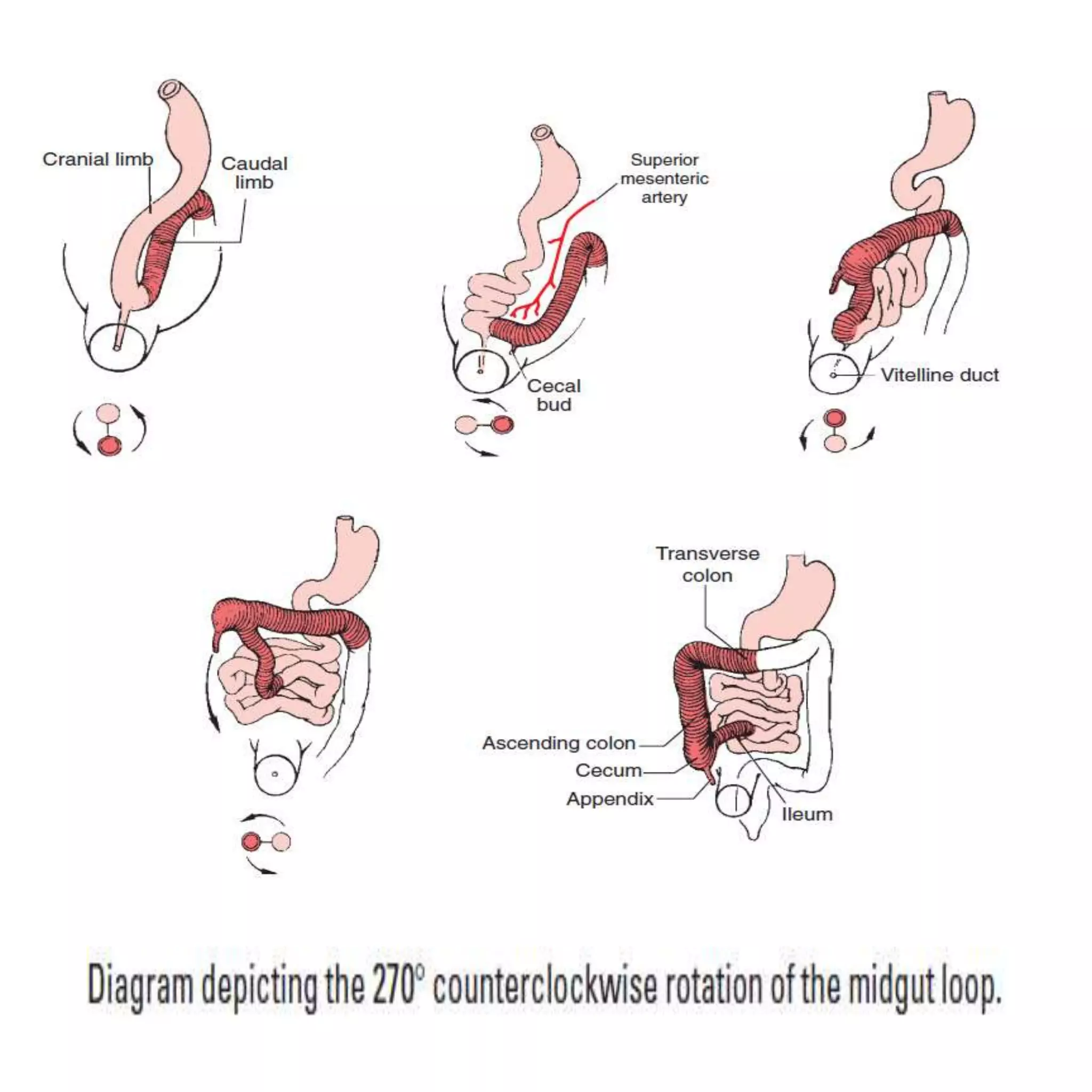
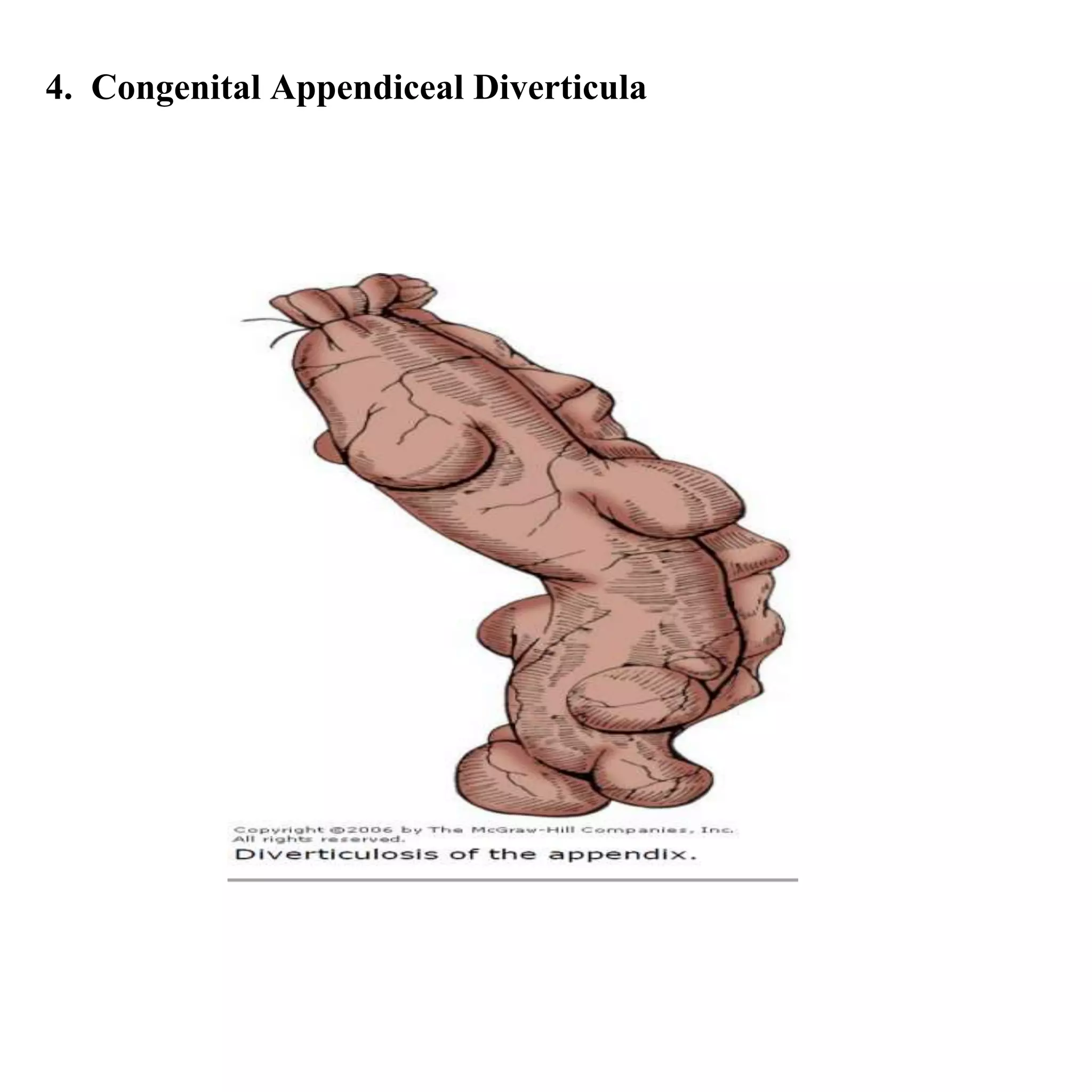
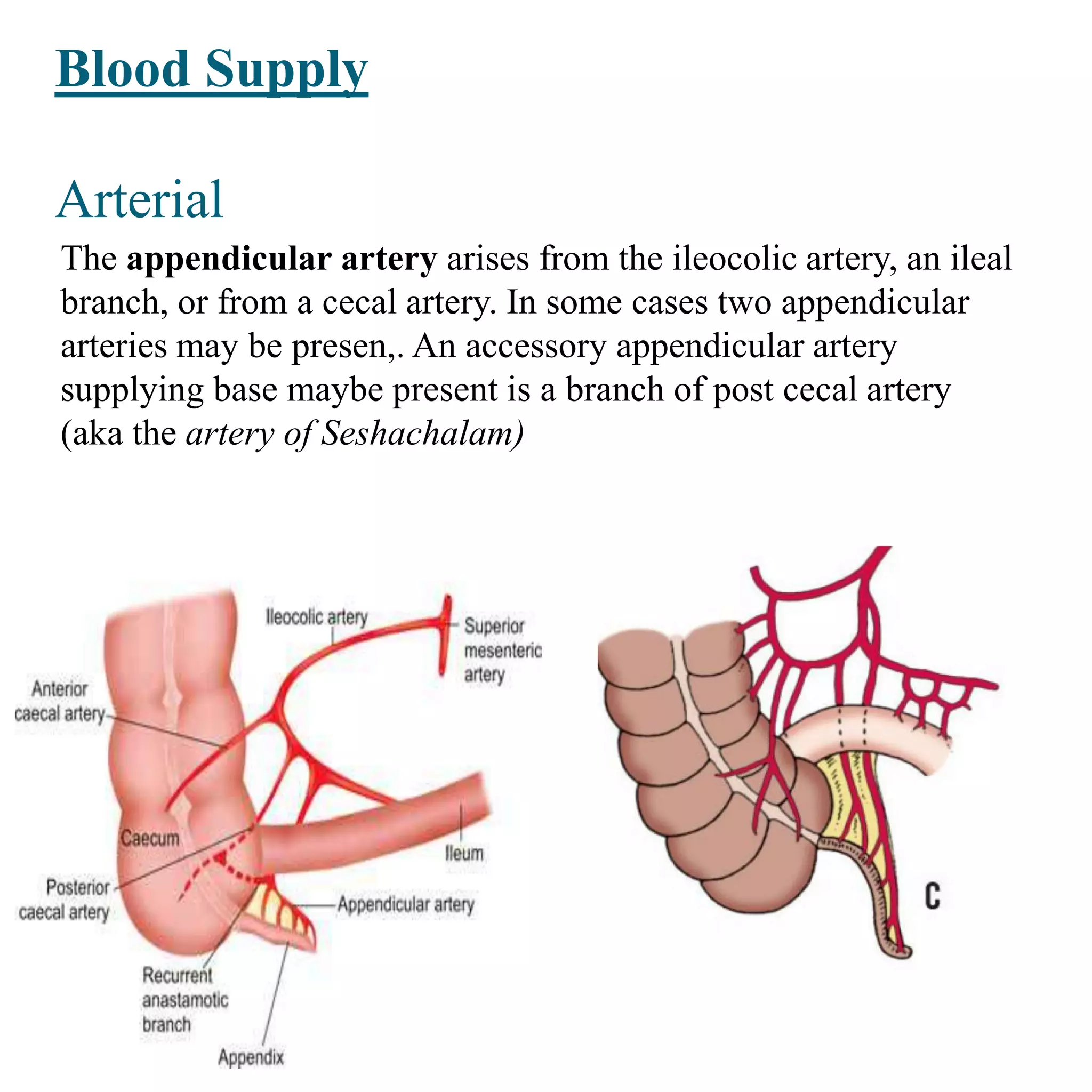
2. The normal anatomy and variations of the appendix, including its embryonic development, typical size and position, blood supply, and lymphatic drainage.
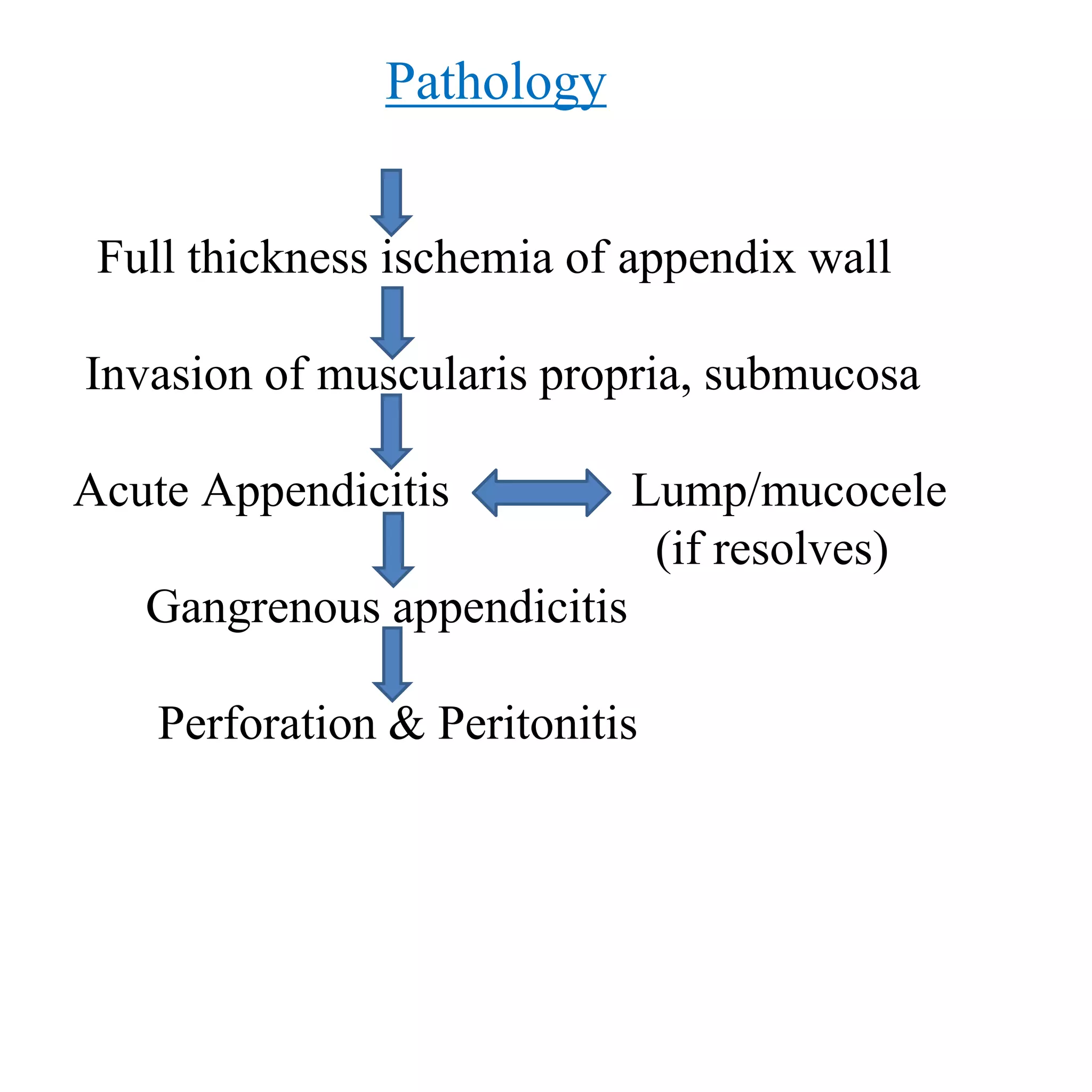
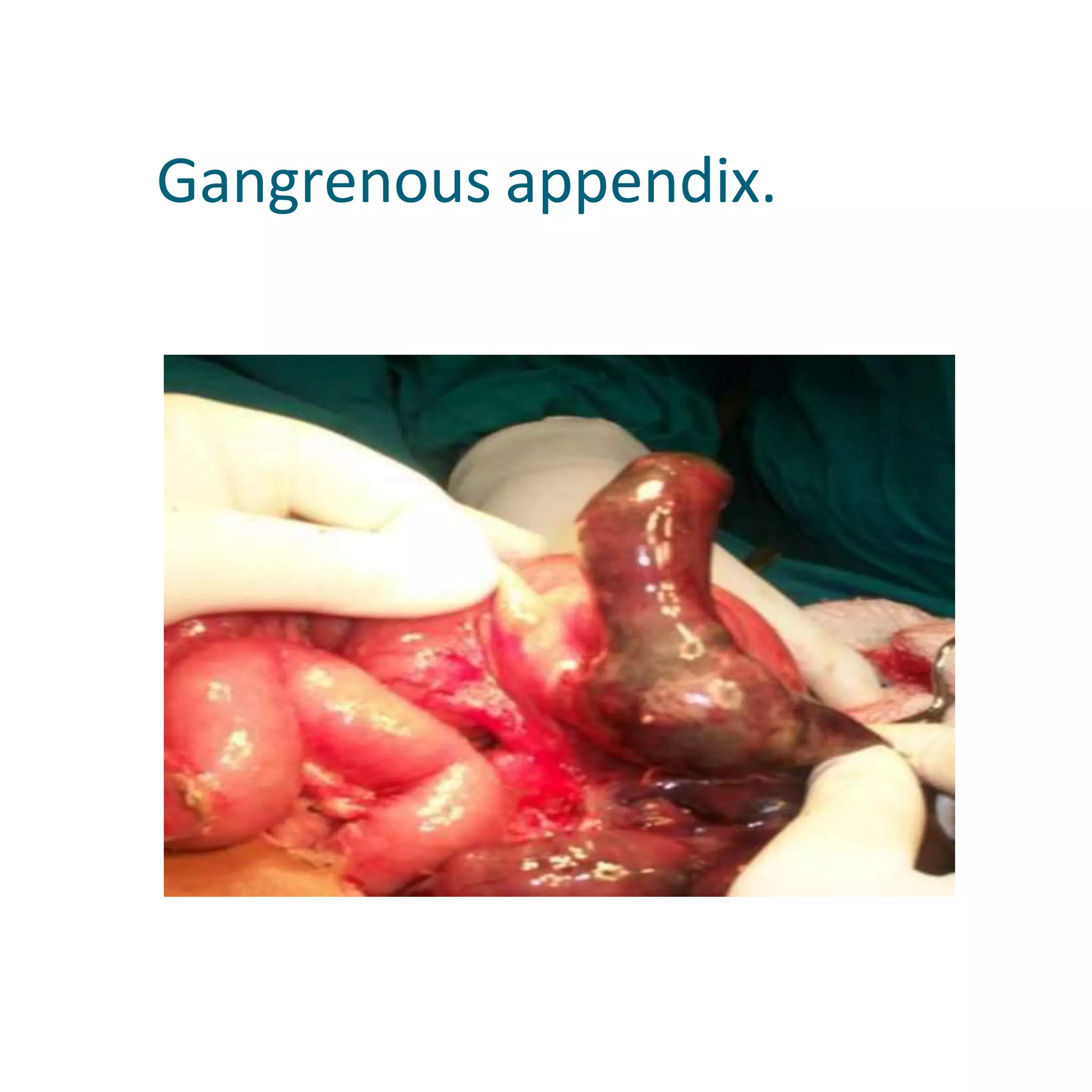
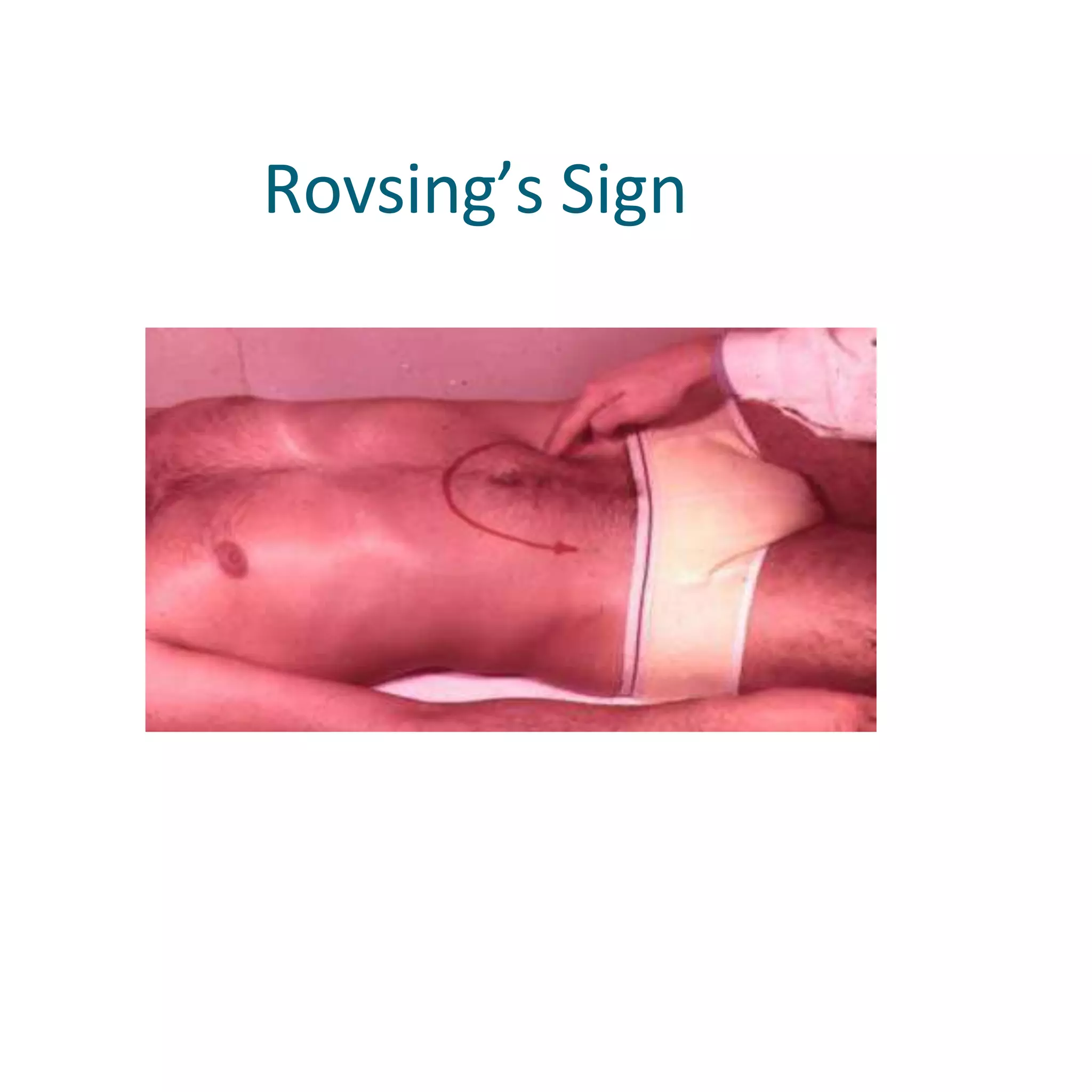
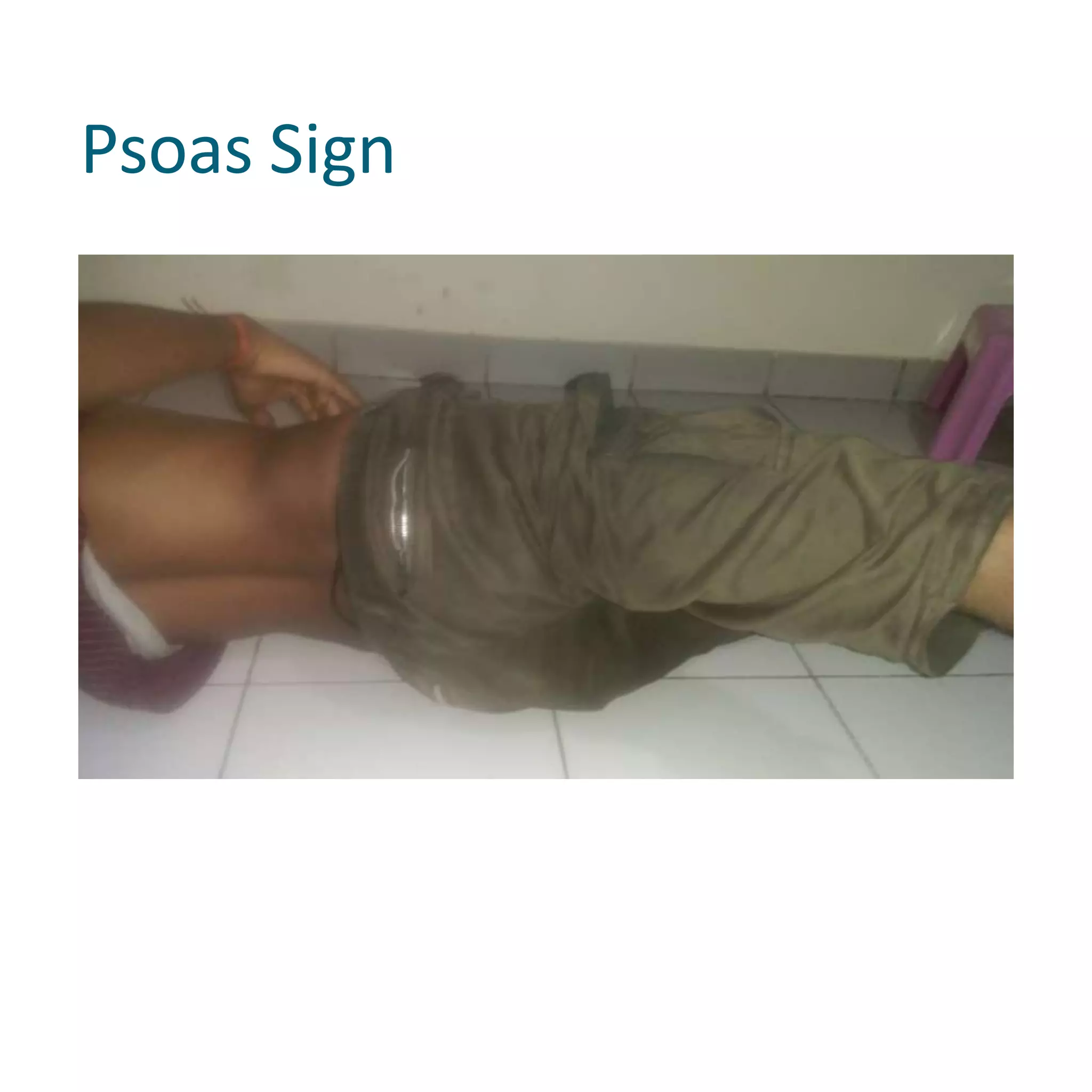
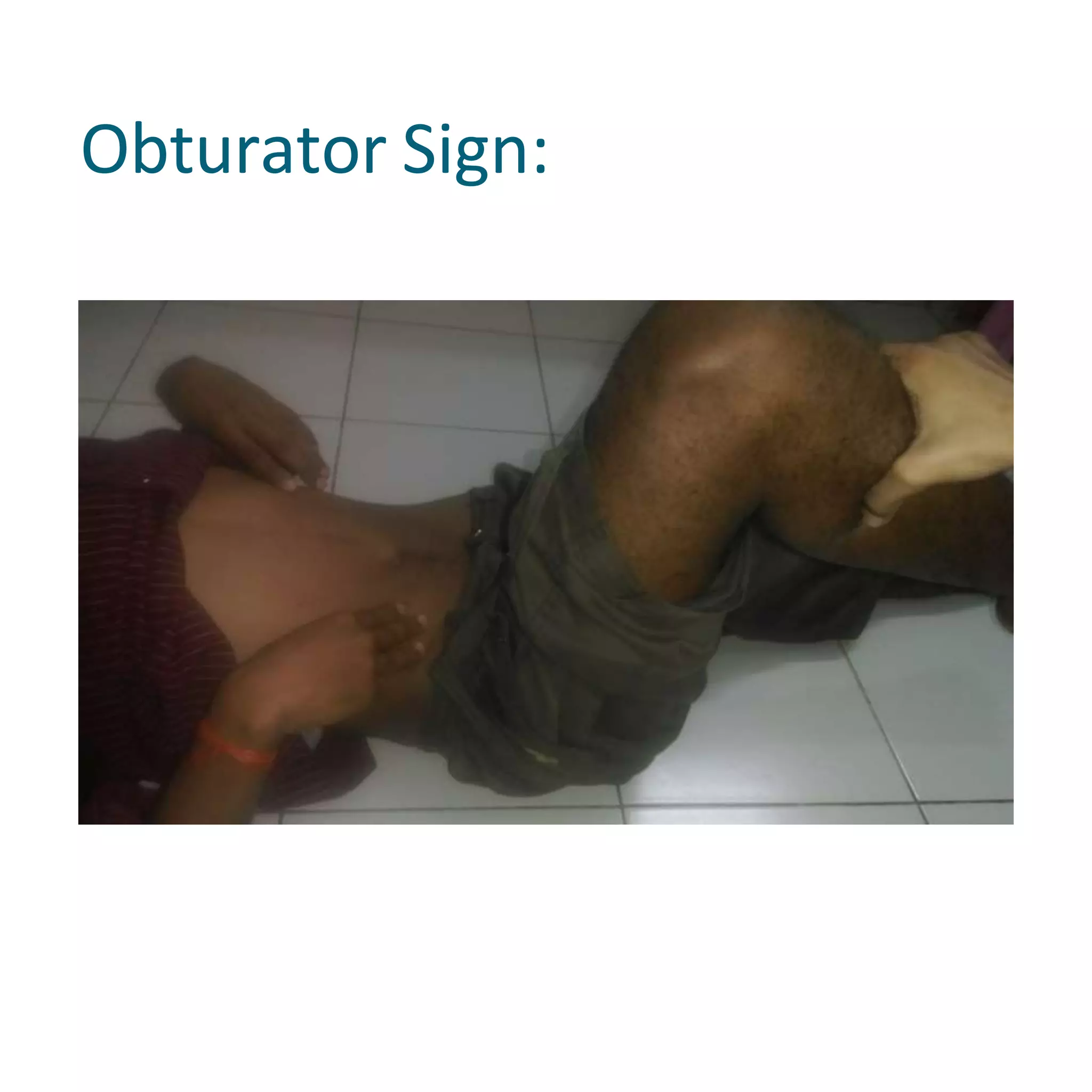
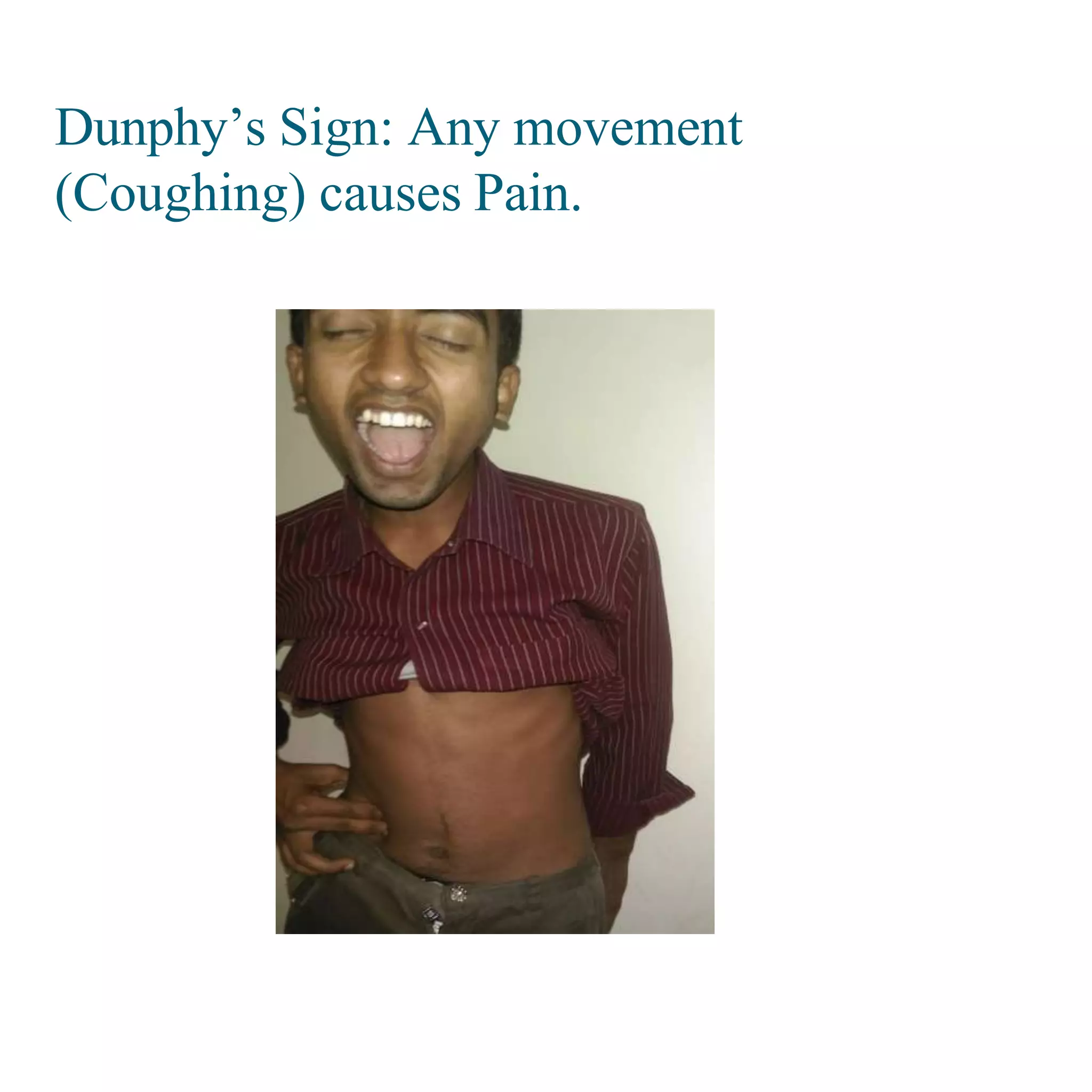
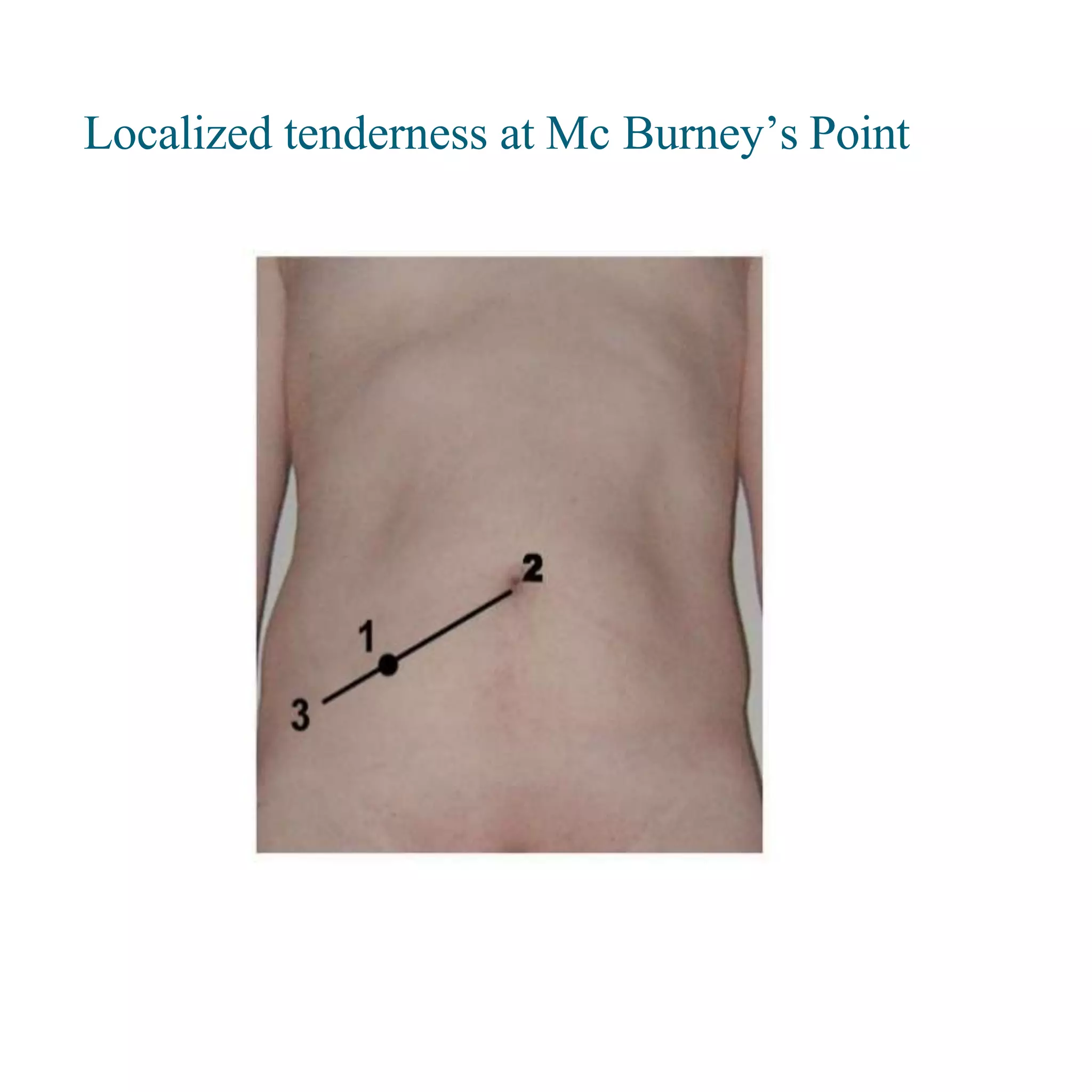
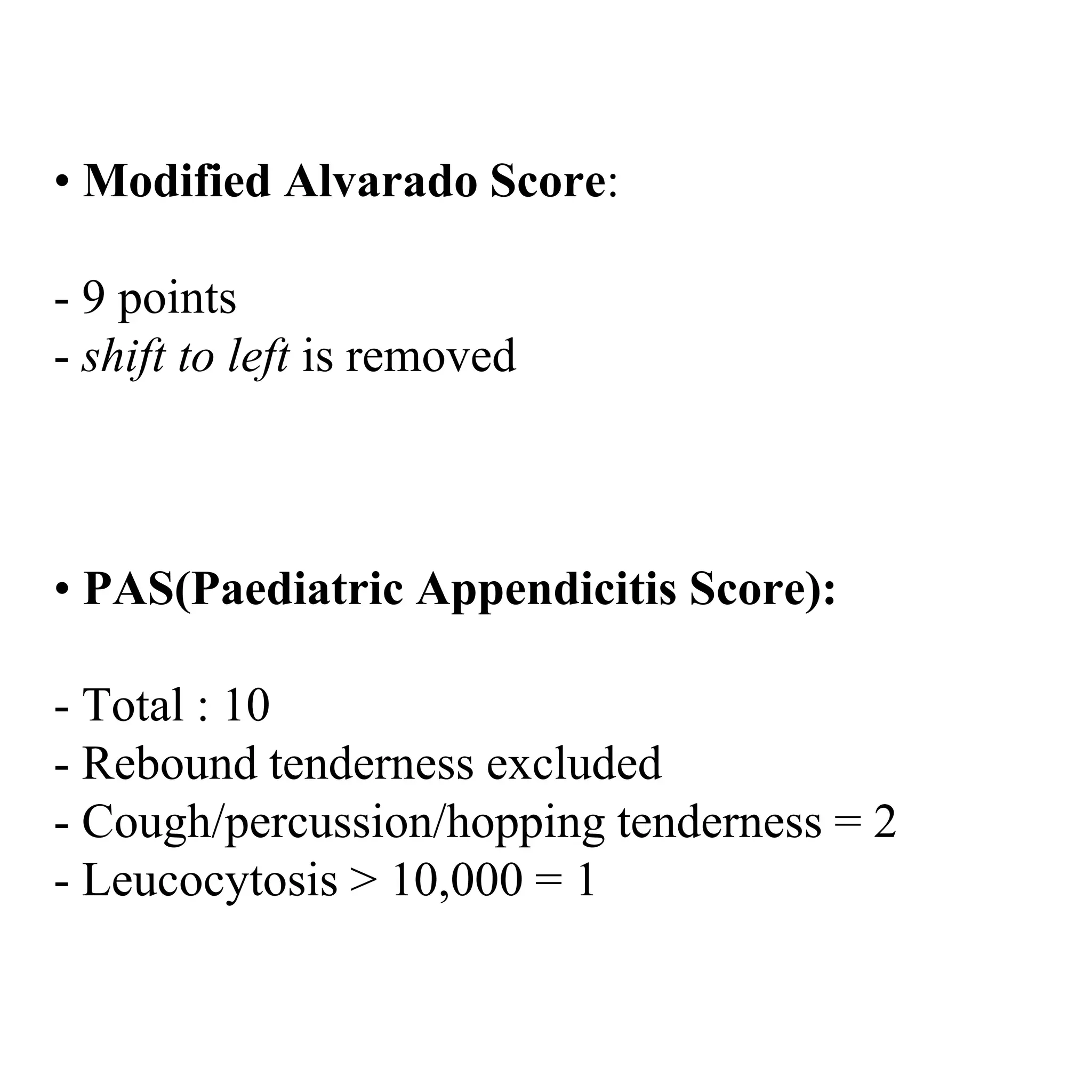
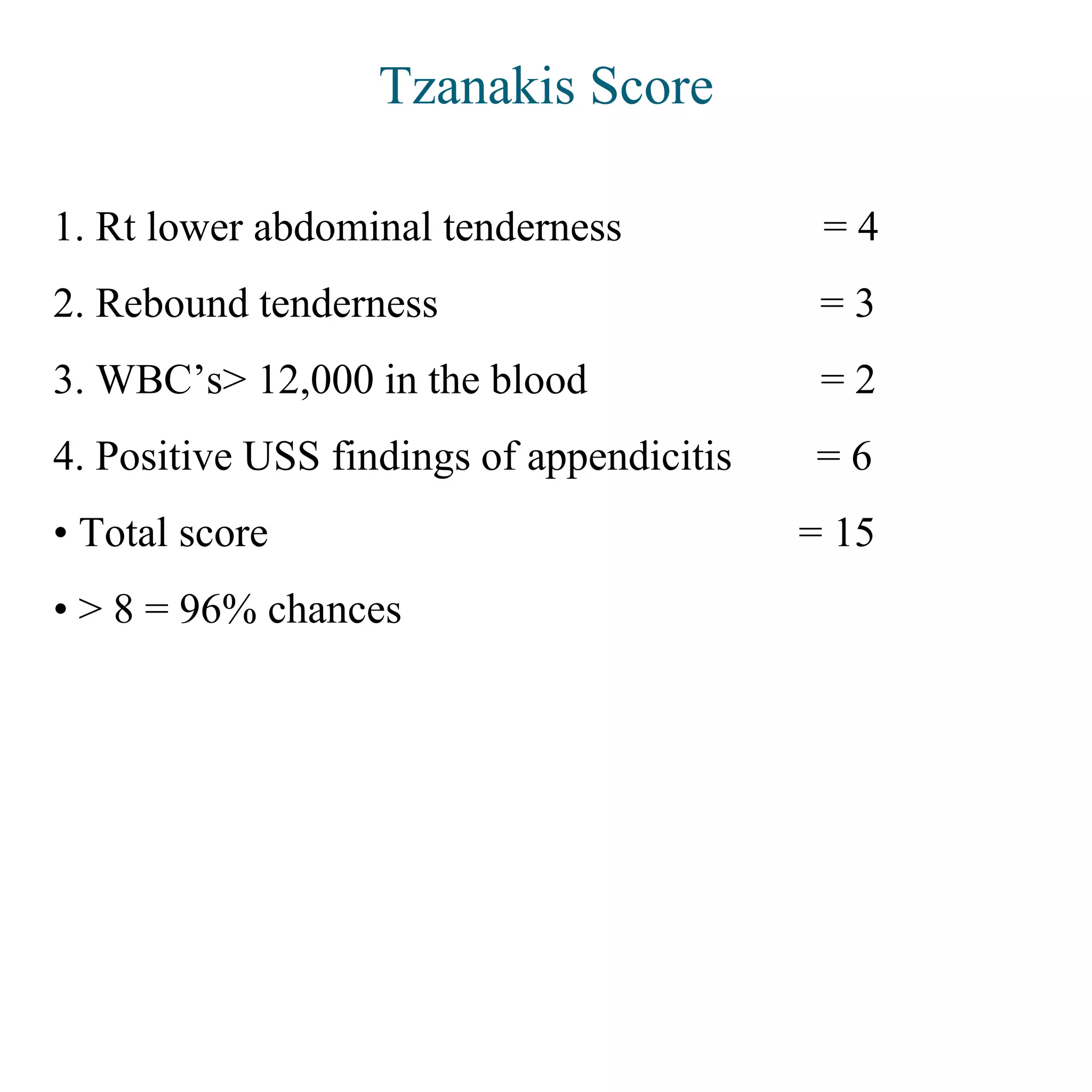
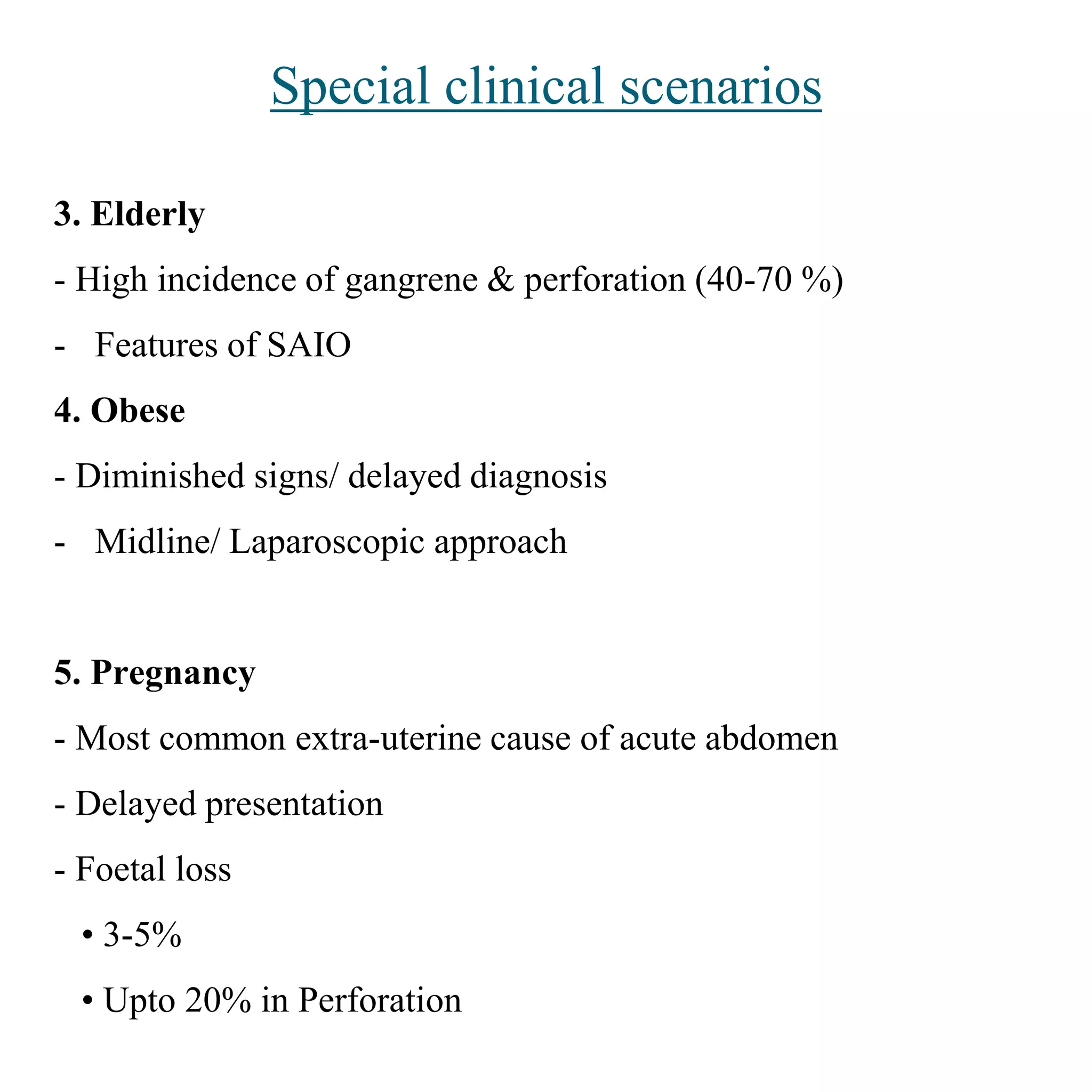
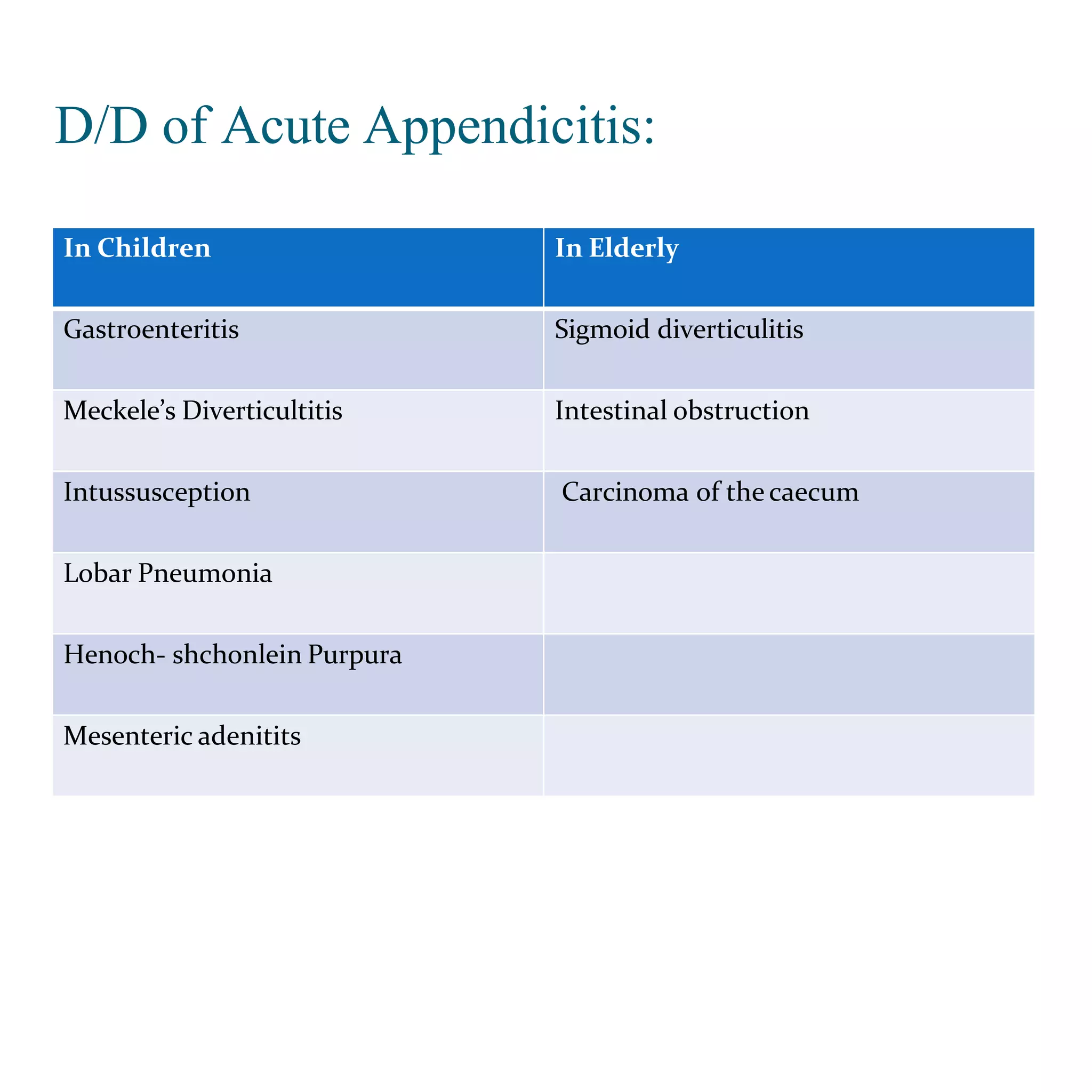
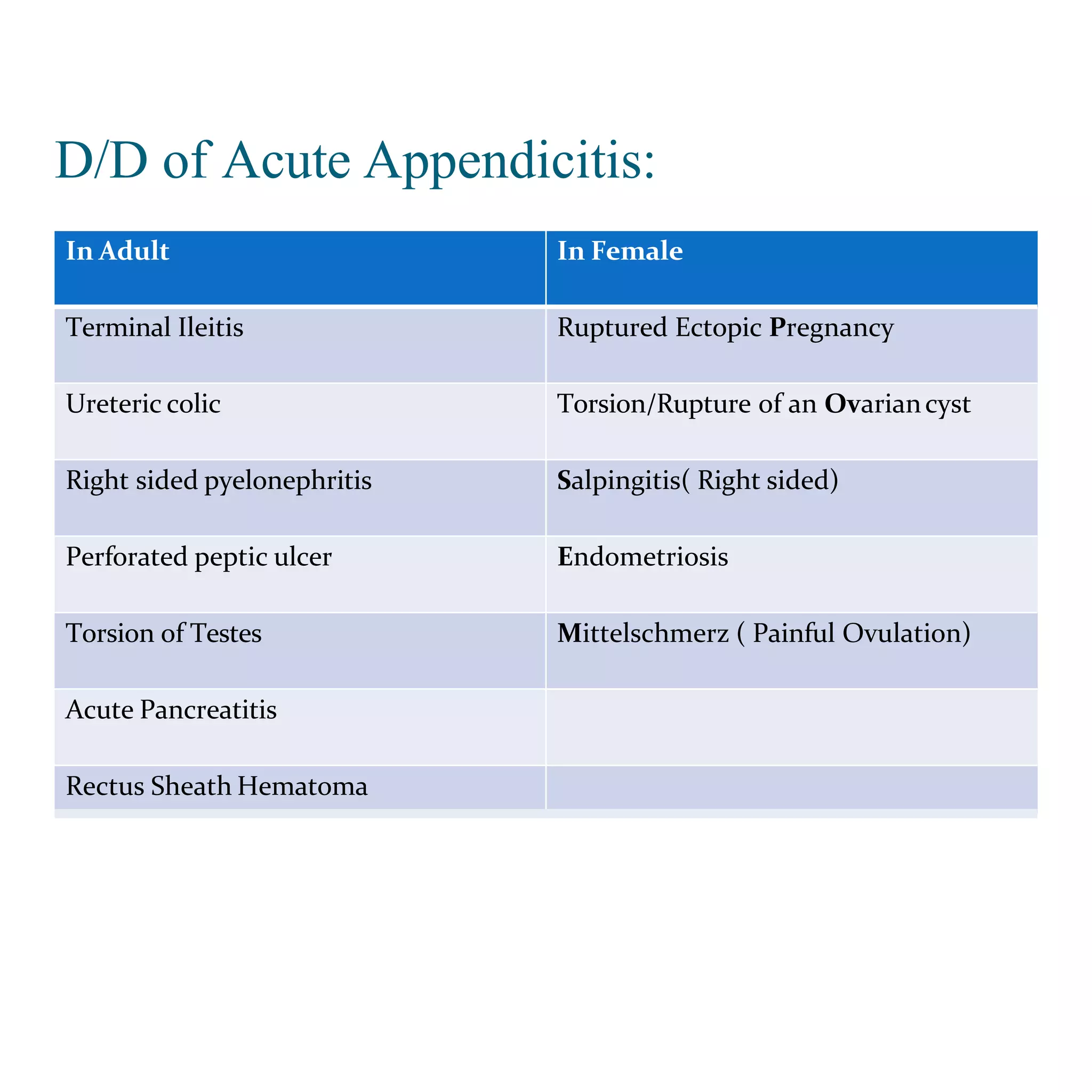
3. The etiology, pathology, clinical features, scoring systems, and special considerations for acute appendicitis depending on the position of the appendix or patient age. Key signs include migration of pain, anorexia, nausea, and localized tenderness at McBurney's point.