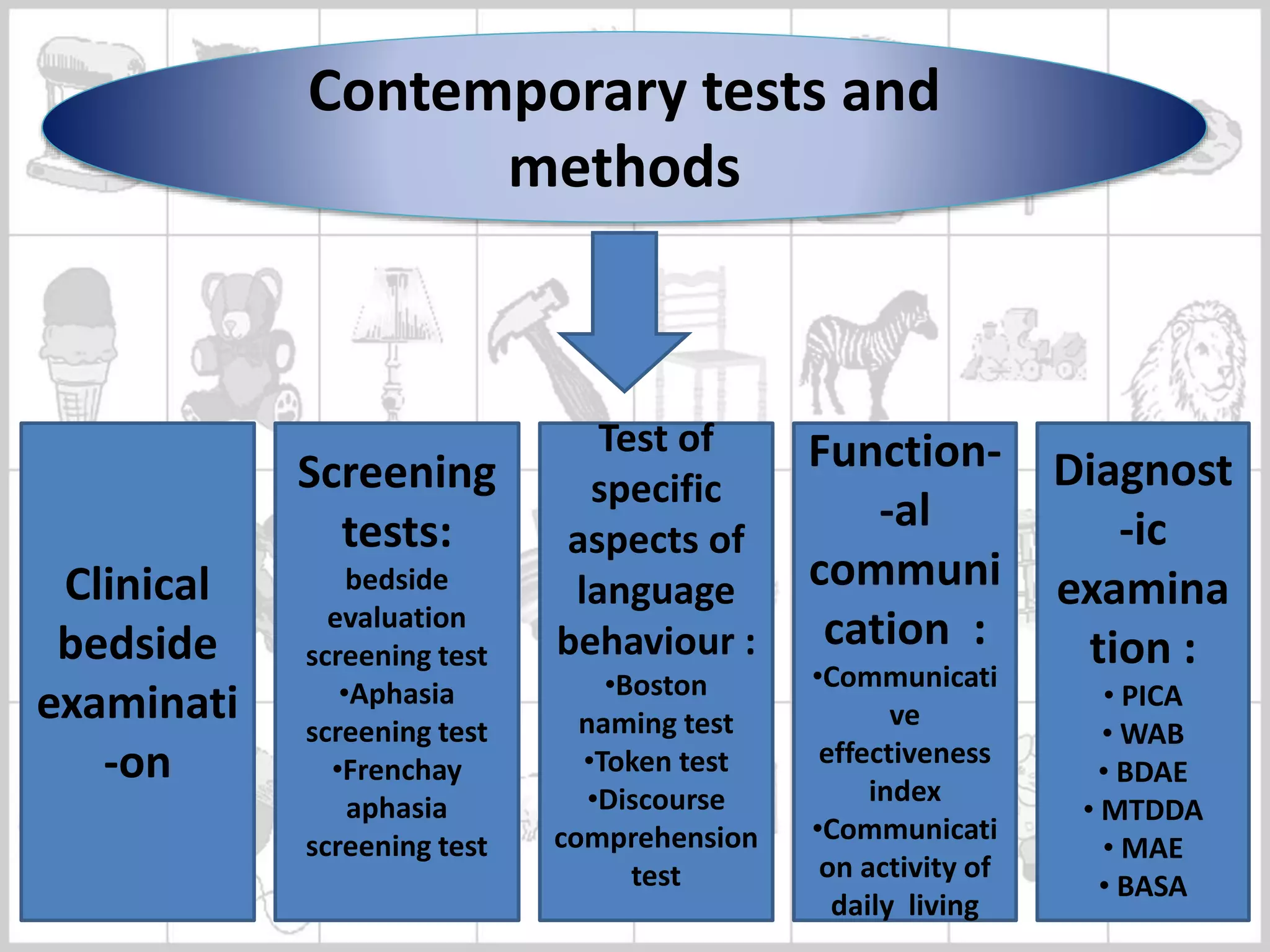
This document presents a case study of a 68-year-old man with aphasia. He had two strokes, in 2010 and 2015, with the second one causing aphasia and a mild phonatory gap. Assessment results showed Broca's aphasia based on limited speech and fair comprehension. On the WAB, he scored 18.9 for aphasia quotient. Voice assessment found hoarseness and a limited pitch range. Therapy was recommended, including speech and language therapy to improve communication and vocal exercises to address the phonatory gap.















![• Speech mechanism ( structure & function ) :
structurally all articulators are normal expect lips,
alternate & lateral movement are affected & jerks
present and all vegetative skills are present but
blowing is affected.
• Perceptual assessment :
Pitch : pitch range is limited, habitual pitch is
high , & pitch breaks are also present
Loudness : very loud
Quality : hoarsness
Phonation duration : for [ a ] is 7.4 sec for [ i ] is 8
sec & for [ u ] is 5 sec.](https://image.slidesharecdn.com/welcometo25thclinicalconference-181111132712/75/aphasia-in-brief-31-2048.jpg)





































































