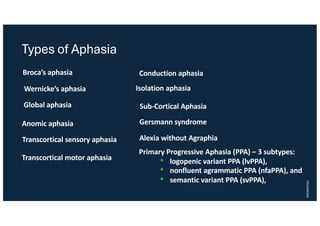
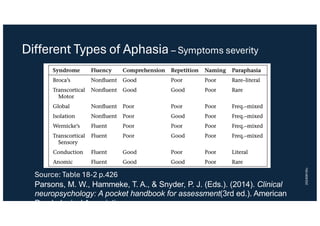
Aphasia is a language impairment caused by functional disruption in specific brain regions, primarily the left hemisphere. Various types of aphasia exist, including Broca's and Wernicke's aphasia, each with distinct symptoms and recovery potential influenced by the injury's type and extent. Rehabilitation strategies encompass speech therapy and understanding brain plasticity, with outcomes varying from rapid recovery to persistent disabilities.


![[INFOGRAPHIC] Understanding Aphasia](https://cdn.slidesharecdn.com/ss_thumbnails/aphasia-130729151927-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)














































