





























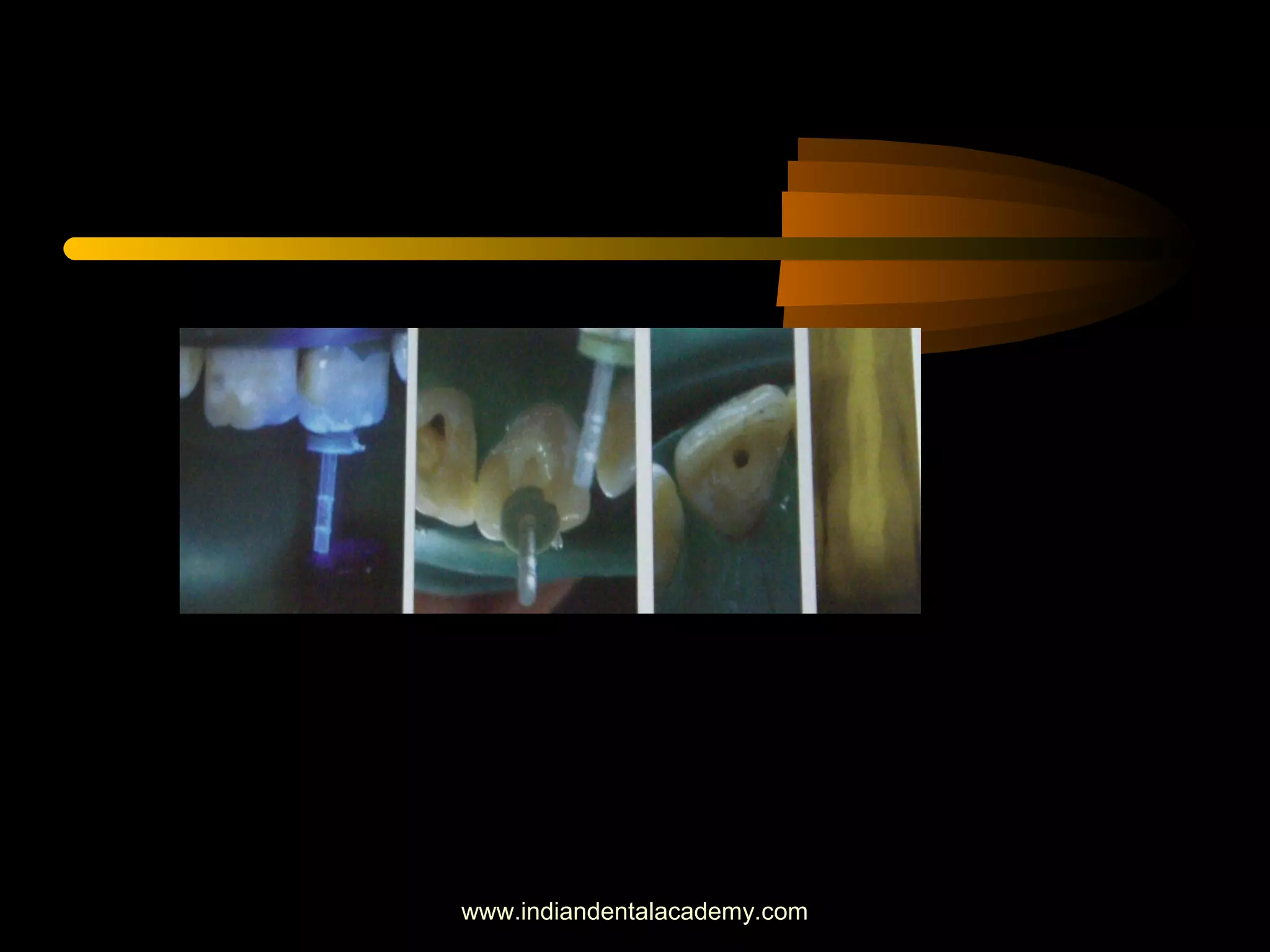
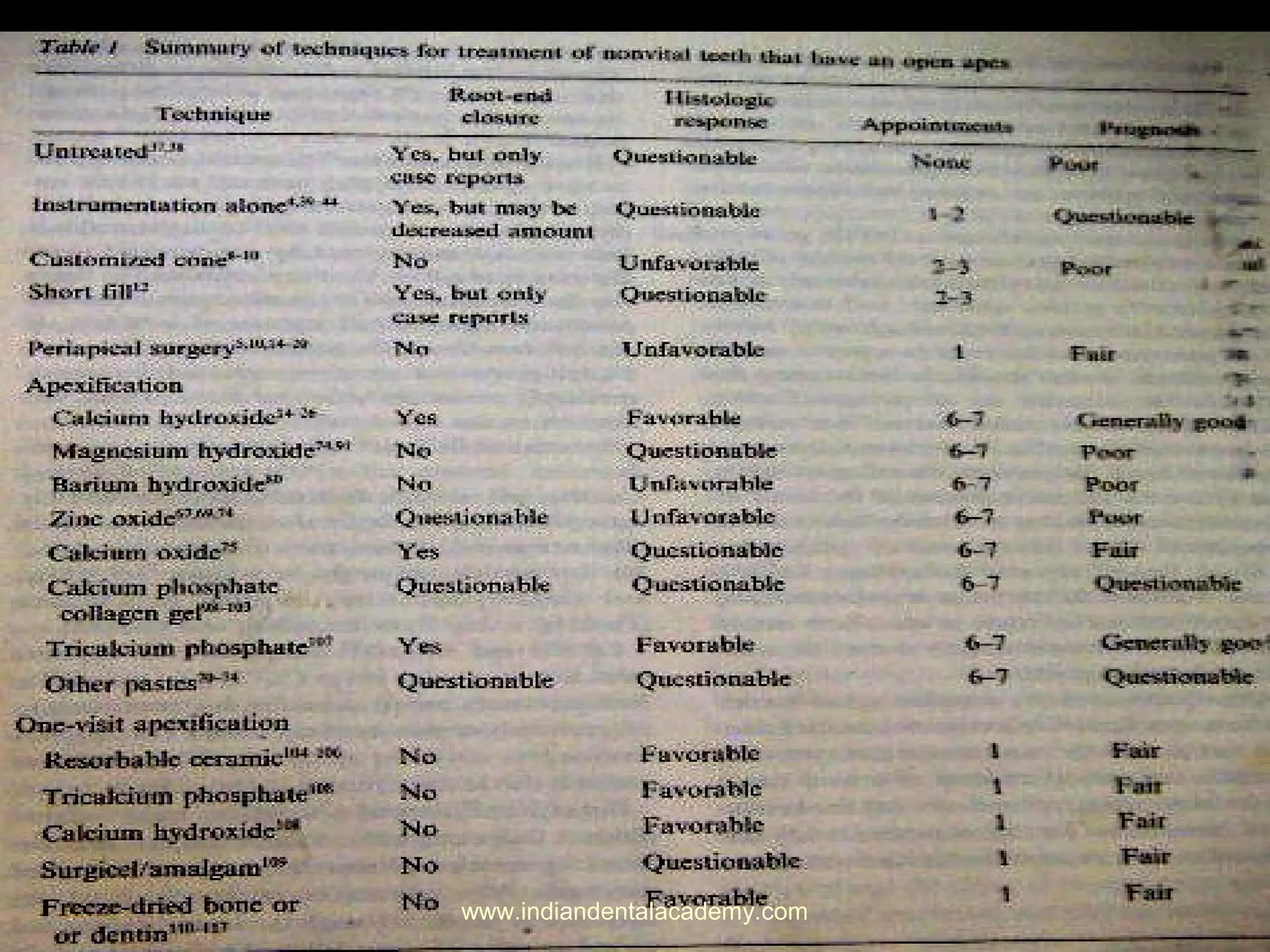



The document discusses apexification, a dental procedure used to encourage continued root development or induce formation of a calcified barrier in a tooth with an open apex or incomplete root formation. It reviews various treatment modalities for apexification including the traditional calcium hydroxide method requiring multiple visits over many months and more recent one-visit methods using biocompatible materials like mineral trioxide aggregate which can induce apical closure in a single appointment. The document provides details on the clinical protocols and materials used for different apexification techniques.























































































