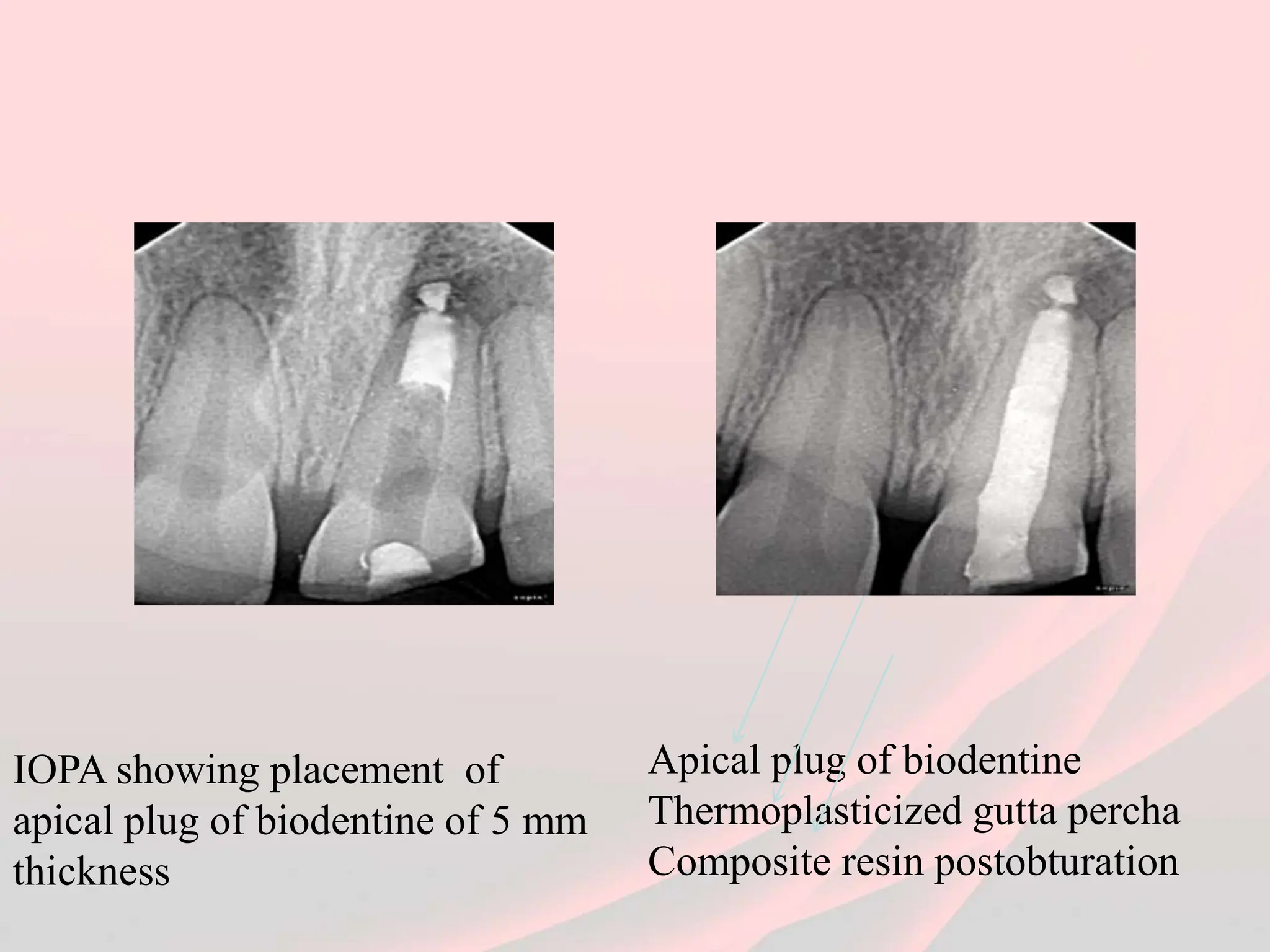
This document details a case study focused on apexification using biodentine for a patient with an immature root apex and pulp necrosis. It highlights the assessment, treatment plan, and subsequent healing process, emphasizing that biodentine facilitates quicker apical barrier formation and healing. The conclusion supports biodentine as a predictable alternative to traditional methods in managing such dental cases.