Downloaded 172 times
![Biological Factors
• benzodiazepines and the azaspirones (e.g.,
buspirone [BuSpar]) have focused biological
research efforts on the γ-aminobutyric acid
and serotonin neurotransmitter systems
• Benzodiazepines (which are benzodiazepine
receptor agonists) are known to reduce
anxiety](https://image.slidesharecdn.com/anxietydisorder-130129082120-phpapp01/85/Anxiety-disorder-6-320.jpg)
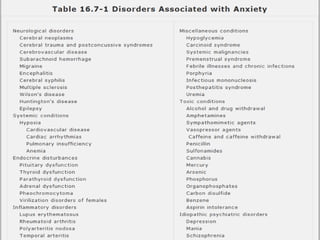
![Etiology
• as amphetamine, cocaine, and caffeine, have
been most associated with the production of
anxiety disorder symptoms, many
serotonergic drugs (e.g., lysergic acid
diethylamide [LSD] and
methylenedioxymethamphetamine [MDMA])
can also cause both acute and chronic anxiety
syndromes in users
• wide range of prescription medications](https://image.slidesharecdn.com/anxietydisorder-130129082120-phpapp01/85/Anxiety-disorder-23-320.jpg)
![Treatment
• the anxiolytic drugs, some data indicate that
the use of triazolobenzodiazepines
(e.g., alprazolam [Xanax]) may be indicated
because of their effectiveness in treating
depression associated with anxiety](https://image.slidesharecdn.com/anxietydisorder-130129082120-phpapp01/85/Anxiety-disorder-34-320.jpg)

Generalized Anxiety Disorder is a common condition affecting 3-8% of the population annually. It involves excessive, uncontrollable worry about everyday life events. Biological factors like the GABA and serotonin systems are involved. Treatment involves psychotherapy, pharmacotherapy like SSRIs, and lifestyle changes. The disorder commonly co-occurs with other conditions like depression and is more prevalent in women. Medical conditions can also cause anxiety disorder-like symptoms.




































































![Chapter 39 role of radiotherapy in benign diseases.pptx [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter39roleofradiotherapyinbenigndiseases-191105205437-thumbnail.jpg?width=640&height=640&fit=bounds)


















