Generalized Anxiety Disorder (GAD) is marked by excessive and unrealistic worry about daily life events, with symptoms affecting concentration, restlessness, and sleep disturbances. It is influenced by genetic, environmental, and biological factors, often treated through psychotherapy and medications like benzodiazepines or buspirone. GAD affects 0.9% of adolescents and 2.9% of adults in the U.S, with higher prevalence in females and those from developed countries.


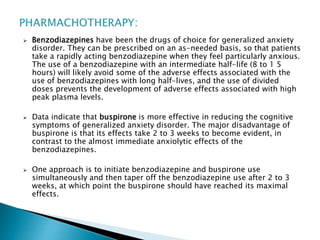
![D. The anxiety, worry, or physical symptoms cause clinically
significant distress or impairment in social, occupational, or
other important areas of functioning.
E. The disturbance is not attributable to the physiological effects
of a substance (e.g., a drug of abuse, a medication) or another
medical condition (e.g., hyperthyroidism).
F. The disturbance is not better explained by another mental
disorder (e.g., anxiety or worry about having panic attacks in
panic disorder, negative evaluation in social anxiety disorder
[social phobia], contamination or other obsessions in
obsessive-compulsive disorder, separation from attachment
figures in separation anxiety disorder, reminders of traumatic
events in posttraumatic stress disorder, gaining weight in
anorexia nervosa, physical complaints in somatic symptom
disorder, perceived appearance flaws in body dysmorphic
disorder, having a serious illness in illness anxiety disorder, or
the content of delusional beliefs in schizophrenia or delusional
disorder).](https://image.slidesharecdn.com/generalizedanxietydisorder-191029044243/85/Generalized-anxiety-disorder-5-320.jpg)
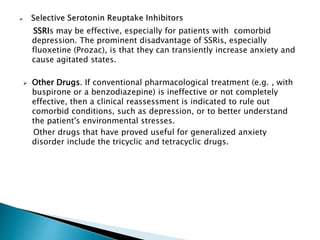
![BIOLOGICAL FACTORS :
The therapeutic efficacies of benzodiazepines and the azaspirones
(e.g., buspirone [BuSpar]) have focused biological research efforts on
the r-aminobutyric acid and serotonin neurotransmitter systems.
Whereas benzodiazepines (which are benzodiazepine receptor
agonists) are known to reduce anxiety, flumazenil (Romazicon) (a
benzodiazepine receptor antagonist) and the /3-carbolines
(benzodiazepine receptor reverse agonists) are known to induce
anxiety.
Some researchers have focused on the occipital lobe, which has the
highest concentrations of benzodiazepine receptors in the brain.
Other brain areas hypothesized to be involved in generalized anxiety
disorder are the basal ganglia, the limbic system, and the frontal
cortex.](https://image.slidesharecdn.com/generalizedanxietydisorder-191029044243/85/Generalized-anxiety-disorder-8-320.jpg)






























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




