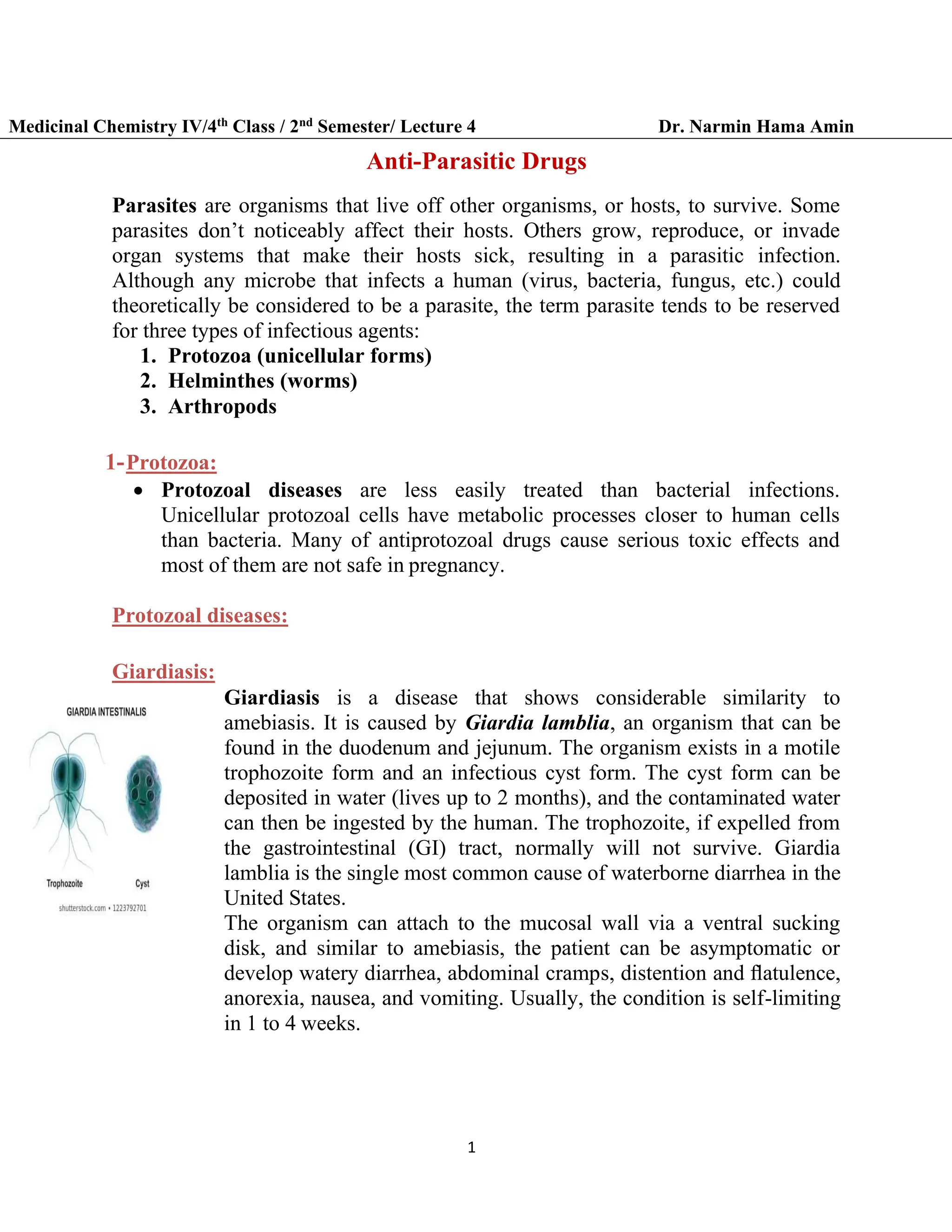
This document summarizes several protozoal diseases and their treatment with anti-parasitic drugs. It discusses the diseases giardiasis and amebiasis caused by the protozoa Giardia lamblia and Entamoeba histolytica respectively. It also discusses trichomoniasis caused by Trichomonas vaginalis. The main drugs used to treat these diseases are metronidazole, tinidazole, and nitazoxanide. It provides details on the mechanisms of action and metabolism of these drugs. It also briefly discusses diloxanide furoate and leishmaniasis.




![6
Medicinal Chemistry IV/4th Class / 2nd Semester/ Lecture 4 Dr. Narmin Hama Amin
the glucuronide, which shows some biologic activity, and small amounts of
an aromatic hydroxylation product.
Metabolic activation of nitazoxanide
Diloxanide Furoate :
▪ Diloxanide furoate (available from the Centers for Disease
Control and Prevention [CDC]) is prescribed
for the treatment of asymptomatic amebiasis but is
ineffective as a single agent for the extraintestinal form of
the disease.
The drug is administered orally and is hydrolyzed in the
gut to give diloxanide, which is considered to be the active drug. Diloxanide
is the only form identifi ed in the bloodstream. The drug is found in the urine
as the glucuronide.
Metabolism of diloxanide furoate](https://image.slidesharecdn.com/antiparasiticdrugs-231126191850-8cb251af/75/Antiparasitic-drugs-Medicinal-Chemistry-6-2048.jpg)




![13
Medicinal Chemistry IV/4th Class / 2nd Semester/ Lecture 4 Dr. Narmin Hama Amin
Trypanosomiasis :
• There are two distinct forms of trypanosomiasis: Chagas disease and
African sleeping sickness.
Chagas Disease :
• Chagas disease, also known as American trypanosomiasis, is caused by the
parasitic protozoa T. cruzi and is found only in the Americas, primarily in
Brazil but also in the southern United States.
• The protozoa lives in mammals and is spread by the bloodsucking insect
known as the reduviid bug, assassin bug, or kissing bug. The insect becomes
infected by drawing blood from an infected mammal and releasing the
protozoa with discharged feces. The pathogen then enters the new host
through breaks in the skin. Inflammatory lesions are seen at the site of entry.
The disease can also be spread through transfusion with contaminated blood.
• Signs of initial infection can include malaise, fever, anorexia, and skin edema
at the site where the protozoa entered the host. The disease ultimately can
invade the heart, where after decades of infection with chronic Chagas
disease, the patient can experience an infection-associated heart attack. It is
estimated that 5% of the Salvadorian and Nicaraguan immigrants to the
United States can have chronic Chagas disease.
African Trypanosomiasis :
• African trypanosomiasis, or sleeping sickness, is caused by several
subspecies of T. brucei (T. brucei rhodesiense [east African sleeping
sickness] and T. brucei gambiense [west African sleeping sickness]). In
this case, the infected animal is bitten by the bloodsucking tsetse fly,
which in turn transmits the protozoa via inoculation during a subsequent
bite of a human.
• The protozoa, initially present in the gut of the vector, appear in the
salivary gland for inoculation during the subsequent biting of a human. It
is estimated that some 50 million people are at risk of African sleeping
sickness, with 300,000 to 500,000 cases occurring in sub-Saharan Africa
each year.
The infection progresses through two stages:
• Stage I can present as fever and high temperatures lasting several days;
hematologic and immunologic changes occur during this stage.
• Stage II occurs after the organism enters the central nervous system
(CNS) and can involve symptoms suggesting the disease name— daytime
somnolence, loss of spontaneity, halting speech, listless gaze, and
extrapyramidal signs (e.g., tremors and choreiform movements). A](https://image.slidesharecdn.com/antiparasiticdrugs-231126191850-8cb251af/75/Antiparasitic-drugs-Medicinal-Chemistry-13-2048.jpg)

![15
Medicinal Chemistry IV/4th Class / 2nd Semester/ Lecture 4 Dr. Narmin Hama Amin
Eflornithine (Ornidyl):
• Metcalf reported the synthesis of eflornithine
(difluoromethyl ornithine [DFMO]) in 1978. Their interest
arose from the desire to prepare ornithine decarboxylase
(ODC) inhibitors as tools for studying the role of polyamines
as regulators of growth processes. ODC catalyzes the
conversion of ornithine to putrescine (1,4-diaminobutane),
which in turn leads to the formation of the polyamines, spermine, and
spermidine. It was not until 1980 that Bacchi demonstrated the potential of
DFMO in the treatment of trypanosomiasis.
• DFMO is a suicide inhibitor of ODC, a pyridoxal phosphate–dependent
enzyme. Evidence suggests that cysteine-360 in ODC is the site of efl
ornithine alkylation (25). Alkylation of ODC blocks the synthesis of
putrescine, the rate-determining step in the synthesis of polyamines.
Mammalian ODC can also be inhibited, but because the turnover of ODC is
so rapid in mammals, eflornithine does not produce serious side effects.
Inhibition of ornithine decarboxylase (Enz-Cys-SH) by eflornithine.](https://image.slidesharecdn.com/antiparasiticdrugs-231126191850-8cb251af/75/Antiparasitic-drugs-Medicinal-Chemistry-15-2048.jpg)


























































































