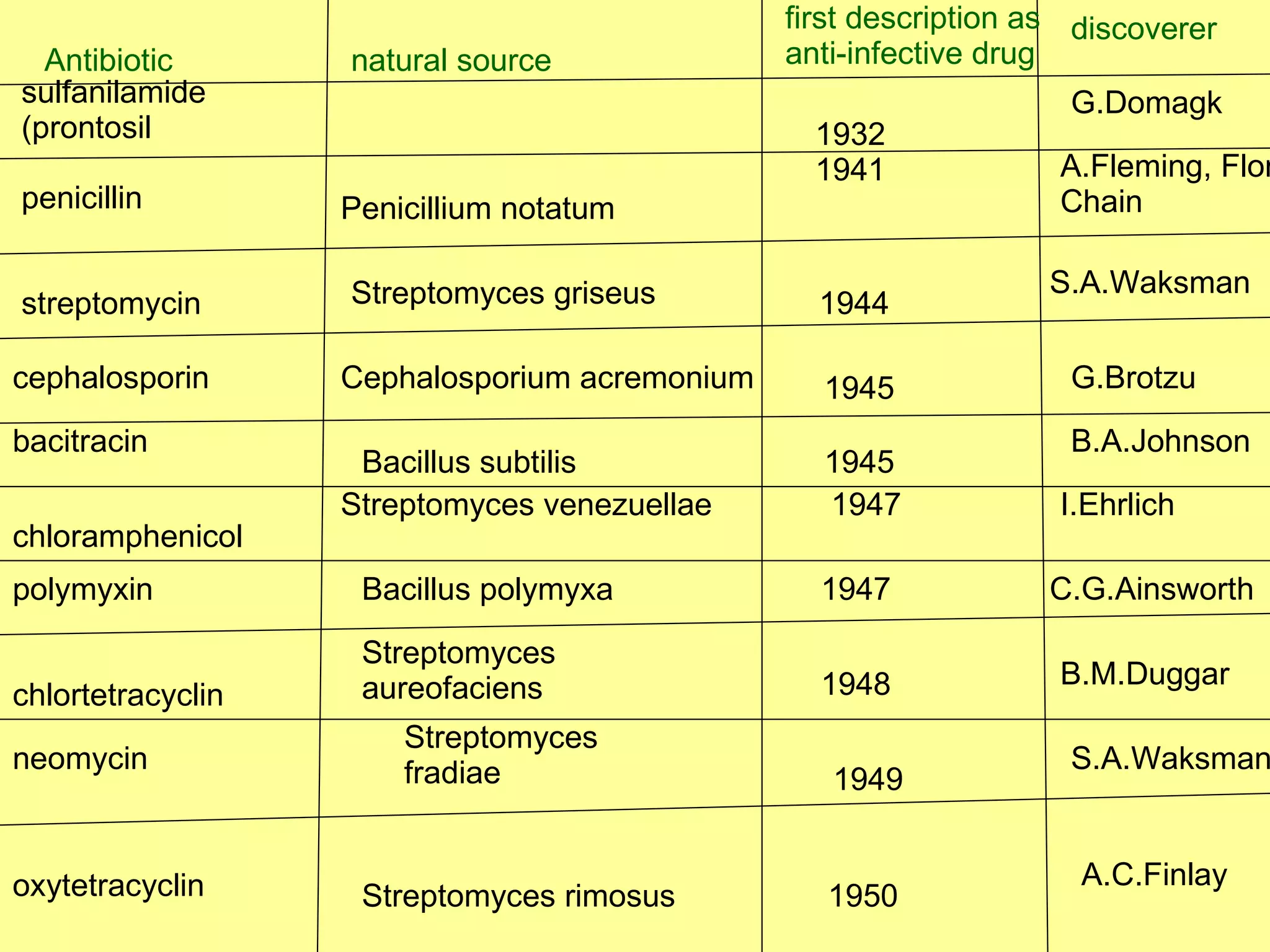
The document discusses the history of antibiotics and antibiotic resistance. It describes some of the key events in the discovery of antibiotics like penicillin and sulfonamides. It also discusses the emergence of resistant bacteria like MRSA and how bacteria can develop resistance through mechanisms such as modifying antibiotic targets, inactivating enzymes, or pumping antibiotics out of the cell. The evolution of antibiotic resistance is an ongoing process driven by selective pressure from antibiotic use.
![Antibiotics – mechanism of resistance – related history [MRSA , VRE , VISA, ESBLS] By Dr.Raghu prakash reddy](https://image.slidesharecdn.com/antibiotic-history-1213966107178635-8/75/Antibiotic-History-1-2048.jpg)























































































![RIFAMPICIN [MEDICINAL CHEMISTRY] BY P.RAVISANKAR.](https://cdn.slidesharecdn.com/ss_thumbnails/rifampicinppt-ravi-copy-130615225737-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)








































