Downloaded 43 times

![Blood schizonticide: Chloroquine
Chloroquine is a synthetic 4-aminoquinoline that has been the
mainstay of antimalarial therapy,
and it is the drug of choice in the treatment of erythrocytic P.
falciparum malaria.
Chloroquine is less effective against P. vivax malaria.
Chloroquine is also effective in the treatment of extraintestinal
amebiasis. [Note: The anti inflammatory action of chloroquine
explains its occasional use in rheumatoid arthritis and discoid lupus
erythematosus.] Chloroquine is a very potent blood
schizonticidal drug , effective against the erythrocytic forms of
all four plasmodial species (if sensitive to the drug), but it does
not have any effect on sporozoites, hypnozoites or gametocytes.
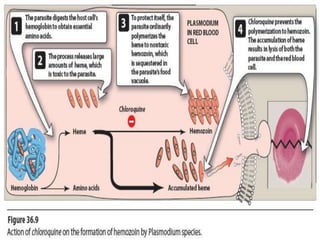
It has a complex mechanism of action that is not fully
understood. It is uncharged at neutral pH and can, therefore,
diffuse freely into the parasite lysosome. At the acid pH of the
lysosome, it is converted to a protonated, membrane-
impermeable form and is 'trapped' inside the parasite.](https://image.slidesharecdn.com/antimalarialdrugs-151126195832-lva1-app6891/85/Antimalarial-drugs-5-320.jpg)
![Adverse effects: Side effects are minimal at the low doses used in
the chemosuppression of malaria.
At higher doses, many more toxic effects occur, such as
gastrointestinal upset, pruritus, headaches, and blurred vision
[Note: An ophthalmologic examination should be routinely
performed.] Discoloration of the nail beds and mucous membranes
may be seen on chronic administration.
Chloroquine should be used cautiously in patients with hepatic
dysfunction or severe gastrointestinal problems and in patients with
neurologic or blood disorders. Chloroquine can cause
electrocardiographic (ECG) changes, because it has a quinidine-like
eff ect.](https://image.slidesharecdn.com/antimalarialdrugs-151126195832-lva1-app6891/85/Antimalarial-drugs-8-320.jpg)

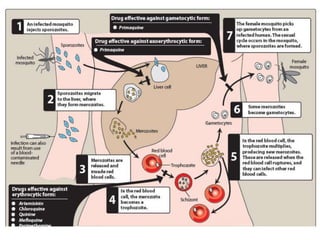
The document discusses various antimalarial drugs, including primaquine, chloroquine, quinine, artemisinin, and pyrimethamine, detailing their mechanisms of action, pharmacokinetics, adverse effects, and issues of resistance. Primaquine targets exoerythrocytic forms, while chloroquine is effective against erythrocytic malaria but has resistance challenges. Quinine is reserved for resistant strains, artemisinin is suitable for severe infections, and pyrimethamine serves both as a schizonticide and sporonticide.



































































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)


















